Chapter: Clinical Pharmacology: Pain medications
Opioid agonists
Opioid agonists
Opioid agonists include:
·
codeine
·
fentanyl
·
hydrocodone
·
hydromorphone
·
levorphanol
·
meperidine
·
methadone
·
morphine sulfate (including morphine sulfate sustained-release tablets
and intensified oral solution)
·
oxycodone
·
oxymorphone
·
propoxyphene
·
remifentanil
·
sufentanil.
Gold standard
Morphine sulfate is the standard against which the
effectiveness and adverse reactions of other pain medications are measured.
(See Using opioid agonists safely.)
Pharmacokinetics
A person may receive an opioid agonist by any
administration route, although inhalation administration is uncommon. Oral
dos-es are absorbed readily from the GI tract; however, transmucosal and
intrathecal opiates are faster-acting.
Speedy delivery
Opioid agonists administered I.V. provide the most
rapid (almost immediate) and reliable pain relief. The subcutaneous (subQ) and
I.M. routes may result in delayed absorption, especially in patients with poor
circulation.
Distribution
Opioid agonists are distributed widely throughout
body tissues. They have a relatively low plasma protein-binding capacity (30%
to 35%).
Metabolism
Opioid agonists are metabolized extensively in the liver. For ex-ample,
meperidine is metabolized to normeperidine, a toxic metabolite with a longer
half-life than meperidine. This metabolite accumulates in patients with renal
failure and may lead to CNS ex-citation and seizures. Administration of
meperidine for more than
48 hours increases the risk of neurotoxicity and seizures from buildup
of normeperidine.
Excretion
Metabolites are excreted by the kidneys. A small
amount is excret-ed in stool through the biliary tract.
Pharmacodynamics
Opioid agonists reduce pain by binding to opiate receptor sites (mu
receptors and N-methyl-D-aspartate
receptors) in the periph-eral nervous system and the CNS. When these drugs
stimulate the opiate receptors, they mimic the effects of endorphins (naturally
occurring opiates that are part of the body’s own pain relief sys-tem). This
receptor-site binding produces the therapeutic effects of analgesia and cough
suppression. It also produces adverse re-actions, such as respiratory
depression and constipation.
Smooth operator
Opioid agonists, especially morphine, affect the
smooth muscle of the GI and genitourinary tracts (the organs of the
reproductive and urinary systems). This causes contraction of the bladder and
ureters. It also slows intestinal peristalsis (rhythmic contractions that move
food along the digestive tract), resulting in constipa-tion, a common adverse
effect of opiates.
Too much of a good thing
These drugs also cause blood vessels to dilate,
especially in the face, head, and neck. In addition, they suppress the cough
center in the brain, producing antitussive effects and causing constric-tion of
the bronchial muscles. These effects can produce adverse reactions if
excessive. For example, if the blood vessels dilate too much, hypotension can
occur.
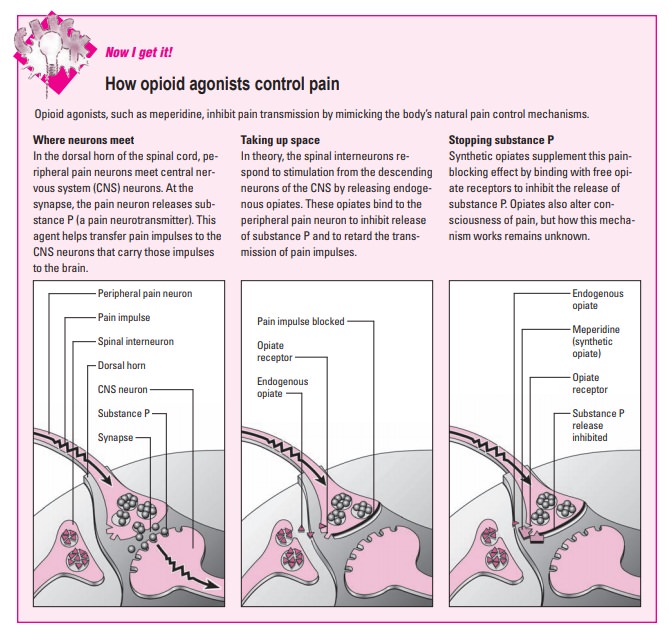
Pharmacotherapeutics
Opioid agonists are prescribed to relieve severe
pain in acute, chronic, and terminal illnesses. They also reduce anxiety before
a patient receives anesthesia and are some-times prescribed to control diarrhea
and suppress cough-ing. (See How opioid
agonists control pain)
Methadone is used for temporary maintenance of
nar-cotic addiction. Other opioids and remifentanil are used for the induction
and maintenance of general anesthesia.
Cardio-assistance
Morphine relieves shortness of breath in patients
with pulmonary edema (fluid in the lungs) and left-sided heart failure
(inability of the heart to pump enough blood to meet the needs of the body). It
does this by dilating peripheral blood vessels, keeping more blood in the
periphery, and decreasing cardiac preload.
Drug interactions
·
The use of opioid
agonists with other drugs that also decrease respirations, such as alcohol,
sedatives, hypnotics, and anesthet-ics, increases the patient’s risk of severe
respiratory depression.
·
Taking tricyclic
antidepressants, phenothiazines, or anticholin-ergics with opioid agonists may
cause severe constipation and urine retention.
·
Drugs that may affect
opioid analgesic activity include amitriptyline, diazepam, phenytoin, protease
inhibitors, and ri-fampin.
·
Drugs that may be
affected by opioid analgesics include carba-mazepine, warfarin, beta-adrenergic
blockers, and calcium chan-nel blockers. (See Adverse reactions to opioid agonists.)
Related Topics