Documentation - Nursing: Records | 11th Nursing : Chapter 13 : Documentation
Chapter: 11th Nursing : Chapter 13 : Documentation
Nursing: Records
Records
Records are one of the essential
components of documentation.
Types of Records
1.
Patients Clinical Records
It is the record of events in the patient illness,
progress in his or her recovery and the type of care given by the hospi-tal
personnel.
2.
Individual staff records.
A separate set of record is needed for staff, giving
details of their absences, their carrier development activities and a personnel
note.
3.
Ward Records
These records are maintained in the each ward, such as
·
Census
records.
·
Change
in medical staff and non nursing personnel for the ward. (Duty roaster)
·
Inventory
and stock records
·
Staffs
Leave records
·
Admission
records
·
Transfer
records
·
Discharge
records
·
Medicine
records etc.
4.
Administrative
records
These records are maintained purely for
administrative purpose of the hospital or unit
·
Legal
documents: for the patients with poisoning, assault, rape, burns etc.
·
Research
or statistics data records
·
Audit
and nursing audit records
·
Quality
of care records
·
Personnel
performance. records
·
Other
administrative records
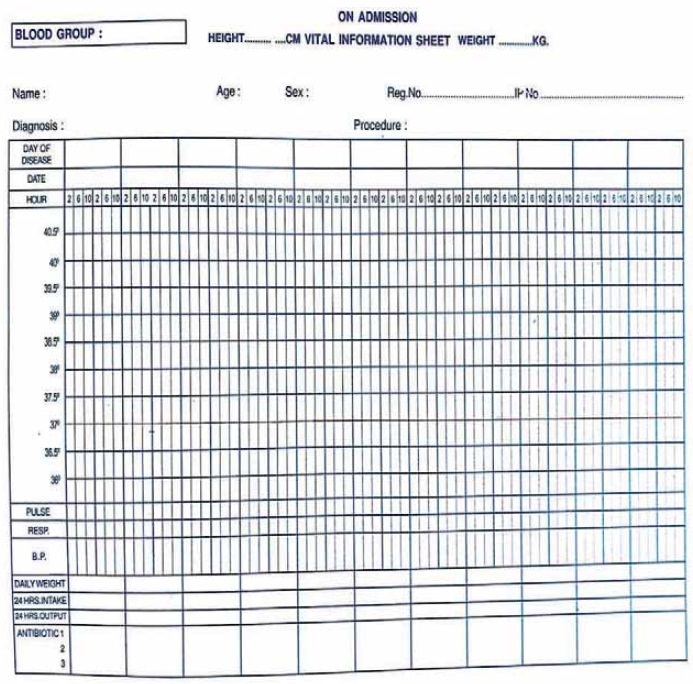
Records Maintained by the Nurses
Vitals sign chart on this the
temperature, pulse and respiration are written in a graphic form so that a
slight deviation from the normal can be noted at a glance
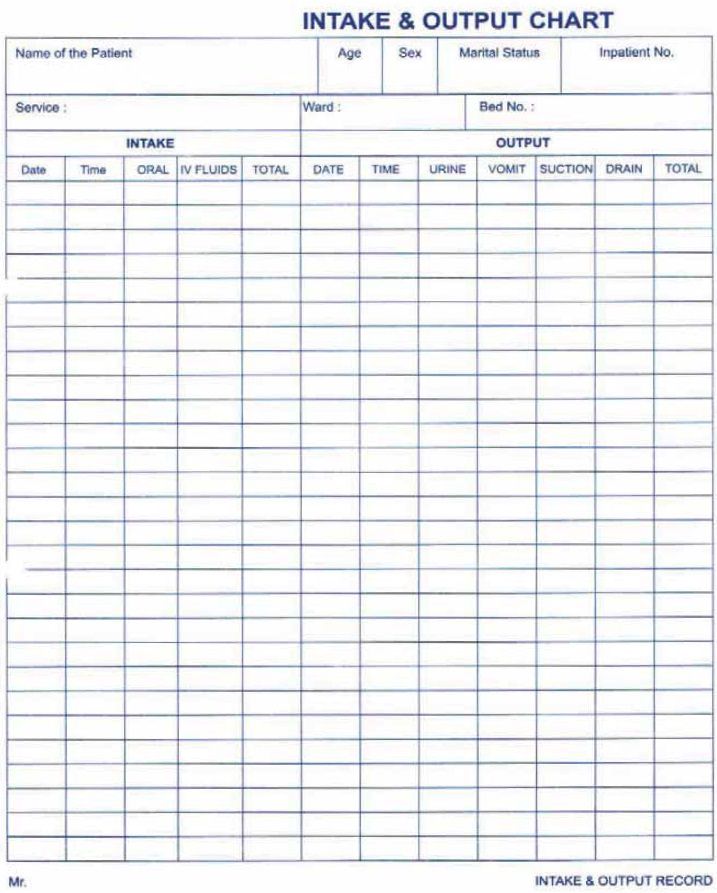
INTAKE AND OUTPUT CHART; Intake and out put chart to be maintained for the
critically ill client those who received intravenous fluids, postoperative
clients, clients with oedema, and client suffering with vomiting and diarrhoea,
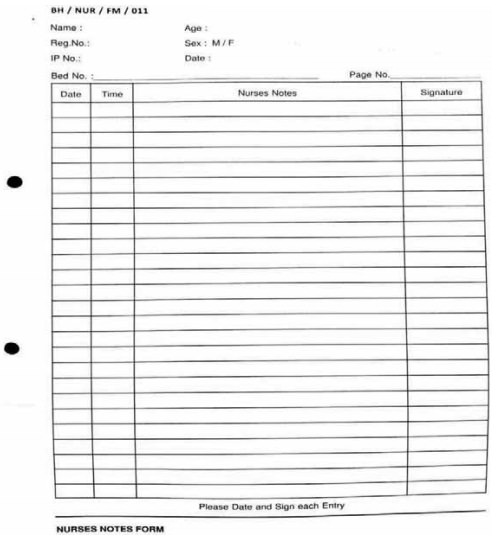
NURSES NOTES.
Nurses notes are a record of
treatments and nursing measures carried out by the nurse which reflects the
observation of the client.
Related Topics