Chapter: Clinical Cases in Anesthesia : Myasthenia Gravis
Following emergence from anesthesia and before extubation, how is strength assessed?
Following
emergence from anesthesia and before extubation, how is strength assessed?
Neuromuscular transmission can be assessed in
many ways. Patients can accomplish sustained head-lift for 5 seconds while 33%
of receptors are still occupied or blocked. Sustained tetanus of 100 Hz for 5
seconds may be seen with 50% of receptors blocked. Negative inspiratory force of
–20 cm H2O also may be accomplished with 50% of receptors occupied.
These measurements of neuromuscular strength suggest that patients can maintain
adequate minute ventilation in the face of residual impairment of neuromuscular
transmission. More recent data suggest that these parameters may not correspond
with the ability to maintain control of the airway. Inspiratory forces of –40
cm H2O may be required to ensure airway control. Other measures such
as tidal volume of 6 mL/kg, TOF >70%, and vital capacity of 15 mL/kg are
relatively insensitive meas-ures of strength.
The myasthenic patient represents a special
case where these numbers may not apply. Their disease, rather than residual
neuromuscular blockade, may prevent myasthen-ics from reaching full strength.
Consequently, preoperative measures of strength are important for postoperative
comparisons. Such tests include negative inspiratory force, maximum breathing
capacity, vital capacity, and tidal volume. Before the administration of an
anesthetic drug that may interfere with neuromuscular transmission, a control
electromyogram or TOF should be recorded. Response to tetanic stimulation
should be assessed after induction of anesthesia and before administration of
drugs that interfere with neuromuscular transmission.
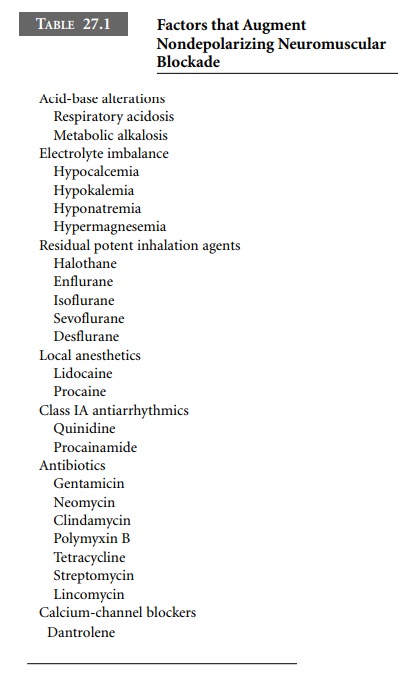
Residual weakness on emergence from anesthesia
must not automatically be assumed to represent residual muscle relaxant
blockade. Inhaled anesthetics, antibiotics, local anes-thetics,
anticonvulsants, and β-blockers may interfere with neuromuscular
transmission (Table 27.1).
Related Topics