Chapter: Clinical Cases in Anesthesia : Total Hip Replacement
Discuss the causes and management of fat embolus syndrome
Discuss the causes and management of fat embolus syndrome.
Microscopic fat emboli are very common in
patients who sustain long bone fractures or who undergo total joint
replacement. Less commonly fat embolus syndrome (FES) may present. It should be
suspected during total joint replacement surgery if the patient develops
hypoxia or agi-tation. FES is present in 0.1% of patients having a total hip
arthroplasty and 7% of patients having a total knee arthro-plasty. It may also
occur during liposuction, osteomyelitis, sickle cell anemia, and burns.
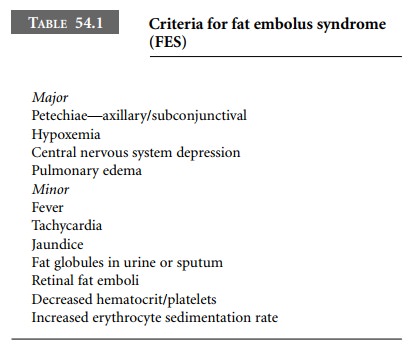
The diagnostic criteria for FES were described
by Gurd (Table 54.1). In order to make the diagnosis, the patient must have one
major and four minor criteria.
There are two theories to describe the
development of FES. One theory postulates a mechanical phenomenon. Fat cells
released into the venous circulation secondary to long bone trauma are
transported to the pulmonary circu-lation where they act as microemboli. The
second theory postulates a biochemical phenomenon. Free fatty acids released
during trauma may directly cause pulmonary damage and adult respiratory
distress syndrome. In addi-tion, the release of stress catecholamines during
trauma results in further free fatty acid release.
There is no definitive treatment for FES. Many
drugs, such as heparin, albumin, and hypertonic glucose, have been used without
success. Steroids may be beneficial in certain high-risk patients. Currently,
supportive measures to maintain hemodynamic stability and optimal oxygena-tion
and ventilation are the only options available. FES usually resolves in 3–5
days.
Related Topics