Chapter: Nutrition and Diet Therapy: Diet and Weight Control
Dietary Treatment of Overweight and Obesity
DIETARY TREATMENT OF
OVERWEIGHT AND OBESITY
Obviously, if a
significant cause of overweight is overeating, the solution is to reduce
portion size and caloric intake. This is seldom easy. To accomplish it, one
must undertake a weight reduction (low-calorie) diet. For the diet to be
effective, one must have a genuine desire to lose weight.
The simplest and,
therefore, perhaps the best weight reduction diet is a normal diet based on
MyPyramid but with the calorie content controlled.
Exchange lists provide
another excellent method to healthfully control the calorie value of the diet.
These lists were originally developed by the American Diabetes Association and
the American Dietetic Association for use with diabetic patients. They are
organized to provide specific numbers of calories and nutrients according to
six lists.
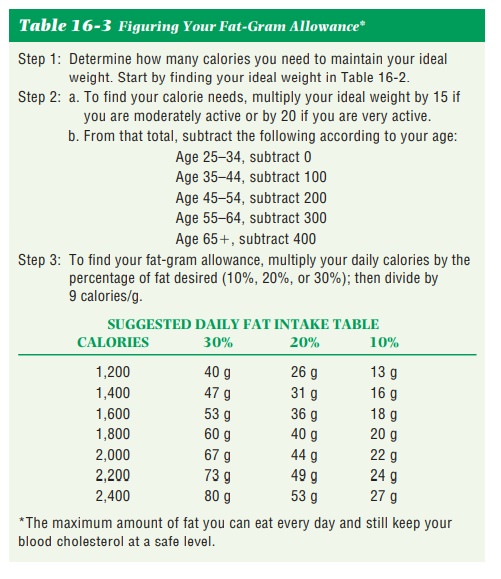
Counting fat grams is
sometimes used to lower calorie intake. Each gram of fat contains 9 calories,
so the reduction of only a few grams of fat per day may result in weight loss.
However, for optimal absorption of fat-soluble vita-mins, one requires that at
least 10% of daily caloric intake come from fats, and 20% to 35% is the
recommended amount for adults. Therefore, in diets limiting fats to 30% of total
calories, one must consume 3 grams of fat per 90 calories; in those limiting
fats to 20% of total calories, one must consume 2 grams of fat per 90 calories;
and in those limiting fats to 10% of total calories, one needs 1 gram of fat
per 90 calories. See Table 16-3 to calculate individual fat-gram allowances.
A reduction of 3,500
calories will result in a weight loss of 1 pound. Physicians frequently
recommend that no more than 1 or 2 pounds of weight be lost in 1 week. To
accomplish this, one must reduce one’s weekly calories (or expend more through
exercising) by 3,500 to 7,000, or daily intake by 500 to 1,000. Diets should
not be reduced below 1,200 calories a day or the dieter will not receive the
necessary nutrients. The diet should consist of 10% to 20% protein, 45% to 65%
carbohydrate, and 20% to 35% or less of fat. In other words, normal proportions
of nutrients but in reduced amounts. The number of meals and snacks each day
should be determined by the dieter’s needs and desires, but the total number of
calories must not be exceeded.
There is no magic way
of losing weight and maintaining the reduced weight, but there is a key to it.
That key is changing eating habits.
In fact, unless eating habits are truly changed, it is likely that the lost weight
will be regained. The cost of slimness is eating less than one might prefer and
exercising most days of the week for 90 minutes.
Food Selection
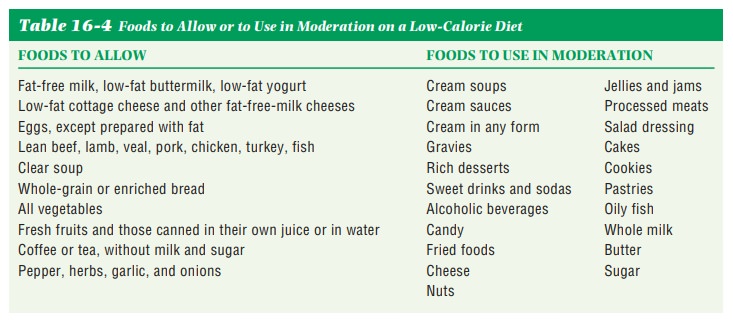
The dieter must learn to “eat smart.” Daily calorie counting is not necessary if one learns the calorie and fat-gram values of favorite foods and considers them before indulging. Some foods are good choices on weight loss diets because of their low-calorie and low-fat-gram values, and some foods should be used in moderation because of their high-calorie and high-fat-gram values (Table 16-4). The low-calorie, low-fat-gram foods should be used during weight loss and thereafter.
Substitutions
of foods with very low calorie contents, preferably nutrient dense, should be
made for those with high-calorie contents whenever possible. The following are
examples:
• Fat-free milk for whole milk
• Evaporated fat-free milk for evaporated milk
• Yogurt or low-fat sour cream for regular sour cream
• Lemon juice and herbs for heavy salad dressings
• Fat-free salad dressings for regular salad dressings
• Fruit for rich appetizers or desserts
• Consommé or bouillon instead of cream soups
• Water-packed canned foods rather
than those packed in oil or syrup
There
are many low-calorie, fat-free, low-fat, sugar-free, and dietetic foods on the
market. A food that is said to be fat-free or sugar-free is not calorie-free.
The food label must be read to determine if the product can fit into a healthy
eating plan for weight reduction. Diet soda can act as a diuretic and can make
one hungry, and it should be used in moderation. Ice water with lemon or lime
slices makes a pleasant calorie-free drink and helps prevent dehydration.
Some
foods that can be eaten with relative disregard for caloric content (provided
they are served without additional calorie-rich ingredients) are listed in
Table 16-5.

Cooking Methods
Broiling, grilling, baking, roasting, poaching, or boiling are the preferred methods because no additional fat is added, unlike frying. Skimming fat from the tops of soups and meat dishes will reduce their fat content, as will trimming fat from meats before cooking. The addition of extra butter or margarine to foods should be avoided and should be replaced with fat-free seasonings such as fruit juice, vinegar, and herbs and spices.
Exercise
Exercise, particularly
aerobic exercise, is an excellent adjunct to any weight loss program. Aerobic
exercise uses energy from the body’s fat reserves as it increases the amount of
oxygen the body takes in. Examples are dancing, jogging, bicycling, skiing,
rowing, and power walking. Such exercise helps tone the muscles, burns
calories, increases the BMR so food is burned faster, lowers the set point, and
is fun for the participant. Any exercise program must begin slowly and increase
over time to avoid physical injuries.
Exercise alone can
only rarely replace the actual diet, however. The dieter should be made aware
of the number of calories burned by specific exercises so as to avoid
overeating after the workout. General daily guidelines for exercise are 30
minutes to prevent chronic diseases, 60 to 90 minutes to prevent weight gain,
and over 90 minutes to maintain weight loss. Children should exercise or be
active 60 minutes every day.
Behavior Modification for Weight Loss
Behavior modification
means change in habits. The fundamental behavior modifications for a weight
loss program are the development of a new and healthy eating plan and an
exercise program that can be used over the long term. These are both major
lifestyle changes, and one may need to participate in a support group or
undergo psychological counseling in order to successfully adapt to these
changes.
It is important that
one learn the difference between hunger and appe-tite. Hunger is the physiological
need for food that is felt 4 to 6 hours after eating a full meal. Appetite is a learned
psychological reaction to food caused by pleasant memories of eating it. For
example, after eating a full meal, one is unlikely to be hungry. Yet when
dessert is served, appetite causes one to want to eat it. One must learn to
listen to one’s body and recognize the difference between hunger and appetite.
Additional behavior modifications are given below.
· Weigh regularly (for
example, once a week), but do not weigh yourself daily.
· Don’t wait too long
between meals.
· Join a support group
and go to meetings during and after the weight loss.
· Eat slowly.
· Use a small plate and
fill it two-thirds with fruits, vegetables, and whole-grain products and just
one-third with meat products.
· Use low-calorie
garnishes.
· Eat whole, fresh foods
that are low-calorie and nutrient-dense. Avoid processed foods.
· Treat yourself with
something other than food.
· Anticipate problems
(e.g., banquets and holidays). “Undereat” slightly before and after.
· “Save” some calories
for snacks and treats.
· If something goes
wrong, don’t punish yourself by eating.
· If there is no weight
loss for 1 week, realize that lean muscle mass is being produced from
exercising or there may be retention of water.
· If a binge does occur,
don’t punish yourself by continuing to binge. Stop it! Go for a walk, to a
movie, to a museum. Call a friend.
· Adapt family meals to
suit your needs. Don’t make a production of your diet. Avoid the heavy-calorie
items. Limit yourself to a spoonful of something too rich for a weight loss
diet. Substitute something you like that is low in calories.
· Take small portions.
· Eat vegetables and bread
without butter or margarine.
· Include daily
exercise. Park further from work and walk.
Patience and
encouragement are needed throughout the adoption of a healthful diet and
exercise regime. Temptation is everywhere, and the dieter should be forewarned.
Just one piece of chocolate cake could set the diet back for half a day
(400–500 calories) and lower resistance to future temptation. Breaking the diet
one day will make it seem easy to break it a second day and so on. Fresh
vegetables and drinks of water may be used to harmlessly prevent or soothe the
hunger pains that are bound to appear. The human body needs at least eight
glasses of water each day, and water can give one a feeling of being full. A
short walk or a few minutes of exercise may help to turn the dieter’s thoughts
from food.
Fad Diets
Many of the countless
fad diets regularly published in magazines and books are crash diets. This means they are
intended to cause a very rapid rate of weight reduction. Often fad diets require the purchase
of expensive foods. Others are part of a weight loss plan including exercise
with special equipment. Expensive food items and equipment can add to the
burden of dieting.
A crash diet usually
does result in an initial rapid weight loss. However, the weight loss is caused
by a loss of body water and lean muscle mass rather than body fat. Sudden
weight loss of this type is followed by a plateau
period; that is, a period in which weight does not decrease.
Disillusionment is apt to occur during this period and may cause the dieter to
go on an eating binge. This can result in regaining the weight that was lost
and sometimes more. This weight gain in turn causes the dieter to try another
weight loss diet, creating a yo-yo effect.
Some popular reducing
diets severely limit the foods allowed, providing a real danger of nutrient
deficiencies over time, and their restricted nature makes them boring. Some
provide too much cholesterol and fat, contributing to atherosclerosis. Some
contain an excess of protein, which puts too great a demand on the kidneys.
Rapid weight loss can cause the formation of gall-stones that could result in
the need for surgery.
These diets ultimately
fail because they defeat the dual purpose of the dieter, which is to lose
weight and prevent its returning. Both can be accom-plished only if eating
habits are changed, and crash diets do not do this.
Surgical Treatment of Obesity
When obesity becomes morbid (damaging to health)
and dieting and exercising are not working, surgery could be indicated. Two of
the surgical procedures used are the gastric
bypass and stomach banding. Both procedures
reduce the size of the stomach.
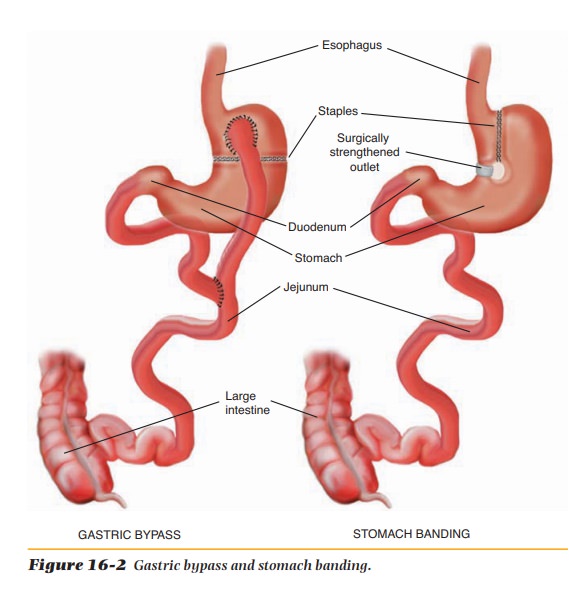
In gastric bypass,
most of the stomach is stapled off, creating a pouch in the upper part. The
pouch is attached directly to the jejunum so that the food eaten bypasses most
of the stomach (Figure 16-2). In stomach banding, the stomach is also stapled
but to a slightly lesser degree than in gastric bypass. The food moves to the
duodenum, but the outlet from the upper stomach is somewhat restricted (Figure
16-2). In both procedures the reduced stomach capacity limits the amount of
food that can be eaten, and fewer nutrients are absorbed. Consequently, weight
is lost.
These procedures are
done only on morbidly obese clients who meet certain strict criteria. A
psychological evaluation will also be given to deter-mine if the client is
ready to change his or her lifestyle and adhere to healthier eating and an
exercise routine. If not, the surgery will not be a success. Also, extensive nutrition
counseling with a dietitian will take place before and after the surgery.
Some obese people may
feel that this surgery would be a quick fix, but it is not. There can be
complications such as bleeding; infections; gastritis; gallstones; and iron,
vitamin B12, and calcium deficiencies. Another common complication
is “dumping syndrome,” which can cause nausea and vomiting, diarrhea, bloating,
and dizziness. Dumping occurs when foods quickly pass into the intestines
without absorption of any nutrients. This happens after partial stomach removal
or small intestine removal, where food (chyme) dumps directly into the large
intestine.
Pharmaceutical Treatment of Obesity
The use of any weight
loss medication, whether by prescription or over the counter, should be
considered very carefully. Miracles are still in short supply.
Amphetamines (pep pills) have been
prescribed for the treatmentof obesity because they depress the appetite.
However, it has been learned that their effectiveness is reduced within a
relatively short time. The dosage must be regularly increased, they cause
nervousness and insomnia, and they can become habit forming. Consequently, they
are rarely prescribed now. Over-the-counter diet pills are available. They are
intended to reduce appetite but are not thought to be effective. In addition to
caffeine and artificial sweet-eners, they contain phenylpropanolamine, which can damage
blood vessels and should be avoided.
Some people believe
that diuretics and laxatives promote weight loss. They do, but only of water.
They do not cause a reduction of body fat, which is what the dieter is seeking.
An excess of either could be dangerous because of possible upsets in fluid and
electrolyte balance. In addition, laxatives can become habit-forming. They
should not be used on any frequent or regular basis without the supervision of
a physician.
Although there is no
magic pill to help those with excess weight reduce, the wish for one remains,
and pharmaceutical companies continue thesearch. Two medications that have
recently been approved by the Food and Drug Administration (FDA) are
sibutramine (Meridia) and orlistat (Xenical). Sibutramine helps to suppress the
appetite and is used in conjunction with a reduced-calorie diet. It is
indicated for those with a BMI of at least 30. Orlistat works in the digestive
system where it blocks about one-third of the fat in food from being digested.
It is recommended that a reduced-calorie diet with no more than 30% from fat be
followed when taking orlistat.
Related Topics