Chapter: Forensic Medicine: Pregnancy-associated deaths
Causes of maternal death
Causes of maternal death
Abortion
Abortion is the expulsion of the product of
conception, and specifically the foetus, from the uterus. According to the
Births and Deaths Registration Act 51 of 1992 a foetus of less than 6 months,
in other words 26 weeks, is not considered to be viable. Any foetus expelled
before a gestational period of 26 weeks is thus by definition an abortion. It
is, however, important to realise that with the help of modern medical
technology such a foetus (or ratherbaby) could survive outside the mother. If
this is the case, this baby is not regarded as an abortion, but as a living
baby and must therefore be registered as such. This apparent contradiction is
not unique to our legal system.
Abortions can be spontaneous or induced.
Spontaneous abortions are a common phenomenon and are often called a
miscarriage. The causes can be maternal, for instance diseases such as fever or
infection, or an anatomically abnormal uterus. The foetus itself may also be
abnormal due to genetic abnormalities. Some women tend to have multiple
abortions, the so-called habitual abortions. These women therefore often have
difficulties in giving birth to a viable baby as they fail to carry the growing
foetus to a fully developed healthy baby at birth.
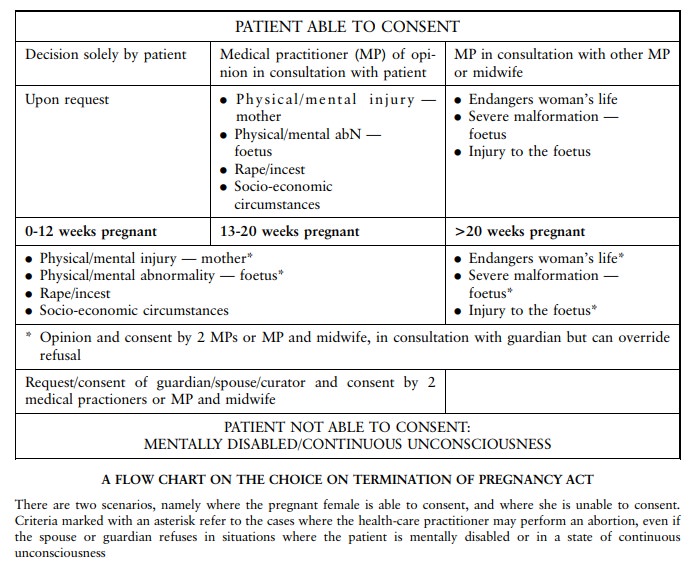
Induced abortions can be therapeutic or criminal.
This is also known as termination of pregnancy. Before the Choice on
Termination of Pregnancy Act 92 of 1996 came into effect on 1 February 1997,
criminal or back-street abortions posed a real and dangerous risk for a
pregnant female wishing to terminate a pregnancy. Approximately 75% of all
deaths associated with abortions were the result of illegal conduct. The old
Abortion and Sterilisation Act, which came into effect in 1975, did allow
therapeutic termination of a pregnancy in certain limited circumstances. It
was, however, not possible for a pregnant female to terminate the pregnancy by
choice.
A therapeutic abortion is associated with
relatively low risk for the mother. The sooner it is performed, the lower the
risk. Criminal abortions, however, have a very high risk, and numerous cases of
death of the mother used to occur. This was also one of the main reasons why
the statutory grounds were broadened and the procedure simplified.
The most important complications of a criminal
abortion are:
·
local inflammation and infection, sometimes complicated by septic shock
·
haemorrhage, followed by hypovolaemic shock
·
neurogenic (nerve) shock, inter alia due to dilatation of the cervix
·
venous air embolism (see study unit 6)
·
the toxic effect of the solutions used to induce the abortion, for
instance soapy solutions
·
amniotic fluid embolism (see study unit 6)
Although the incidence of death due to criminal
abortions has decreased since 1997, criminal abortions are still a real problem.
Any female of child-bearing age who dies suddenly and unexpectedly, must be
regarded as pregnant, and therefore a possible victim of a failed abortion
attempt, until proven otherwise.
Lung embolism
Lung or pulmonary embolism because of a blood
clot (embolus) is a risk during pregnancy and in the puerperium (the period
following termination of pregnancy). Risk factors include operative
intervention, for example caesarean section, or other trauma during delivery,
high maternal age, obesity and any other reason causing the mother to be
immobilised for a period of time.
Amniotic fluid embolism
Amniotic fluid embolism also occurs in full-term
patients. It often occurs in older females who have precipitous labour (ie
where birth is given rapidly).
Injuries and infection
After delivery blood loss due to injuries to the
genital tract may also result in the demise of the patient if not aggressively
managed. Infection is also a risk and puerperal sepsis could develop. As
indicated above, criminal abortions are often complicated by infection or
sepsis.
Pre-eclampsia and eclampsia
Pregnant women can also die due to conditions
unique to pregnancy. With pre-eclampsia there is high blood pressure
(hypertension), oedema and protein in the urine. If the patient develops
convulsions or epileptic fits, it is known as eclampsia. These patients also
have a risk of intracranial haemorrhages (bleeding inside the skull).
Abnormalities of the placenta
Two conditions which may threaten the life of
the mother and the foetus are associated with the placenta.
Late in pregnancy the placenta can become
detached from the uterine wall. Blood-clot abnormalities can develop, and death
could follow. If the baby is not delivered immediately, both the mother and
baby could die. This condition is known as abruptio placentae. In placenta
praevia the placenta is in a low-lying position. With the onset of labour the
cervix or the neck of the uterus dilates. The placenta can then become detached
from the uterine wall, causing possible death of the mother and foetus.
Ectopic pregnancy
Ectopic pregnancy is a condition where the
foetus does not develop in the uterine cavity, but on the outside, often in one
of the Fallopian tubes. When this thin-walled tube ruptures, it could cause
haemorrhage into the abdominal cavity, which could be fatal.
Pre-existing diseases
Pregnancy affects the female body in a number of
ways. It inter alia affects the haemodynamics (circulation and heart). This
hyperdynamic circulation induced by the pregnancy in a female with pre-existing
heart diseases (egvalvular abnormalities) may cause complications and even
death.
Related Topics