Chapter: Modern Medical Toxicology: Organic Poisons (Toxins): Plants of Special Importance
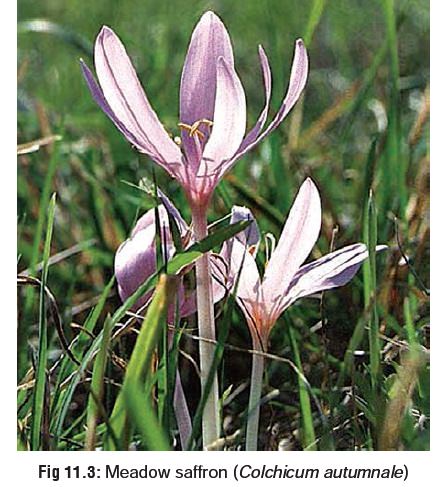
Autumn Crocus(Colchicum autumnale)

Autumn Crocus
Other Common Names
Meadow
saffron; Meadow crocus; Naked lady; Son-before-the-father; Wild saffron.
Botanical Name
Colchicum autumnale.
Physical Appearance
·
It is a perennial plant with whitish
or pale purple flowers (Fig 11.3).
·
The long, broad-lanceolate, dark
green leaves are produced in spring, while the flowers bloom in succession from
August to October, soon dying down.
·
The bulb-like fleshy underground
stems (corms) are about the size of a small tulip bulb, and lie from 6 to 10
inches deep in the soil.
·
This plant grows well in England,
Wales, and many European countries, but is relatively uncommon in Asia. However,
it is encountered in the Himalayan region. The Indian variety usually bears
yellowish flowers.
Uses
■■ The main active principle colchicine is used in the treat-ment of gout. It acts by reducing the inflammatory response to the deposited urate crystals, and also by diminishing phagocytosis. Deposition of urate is favoured by acid pH. Colchicine counters acid pH environment by inhibiting lactic acid production by leucocytes, thereby interrupting urate deposition and inflammatory response that sustains the acute attack.
■■The fruit capsule of Autumn crocus contains numerous dark
brown seeds. The dried capsule is often used as a “rattle” by children. Each
seed contains approximately 3.5 mg of colchicine. Ingestion of 2 seeds may be
poten-tially lethal.
Toxic Part
All
parts, especially fresh corms and ripe seeds.
Toxic Principles
■■Colchicine
■■Demecolcin.
Mode of Action
Colchicine
is an antimitotic agent, blocking mitosis in meta-phase and in the G1
phase, preventing DNA synthesis.
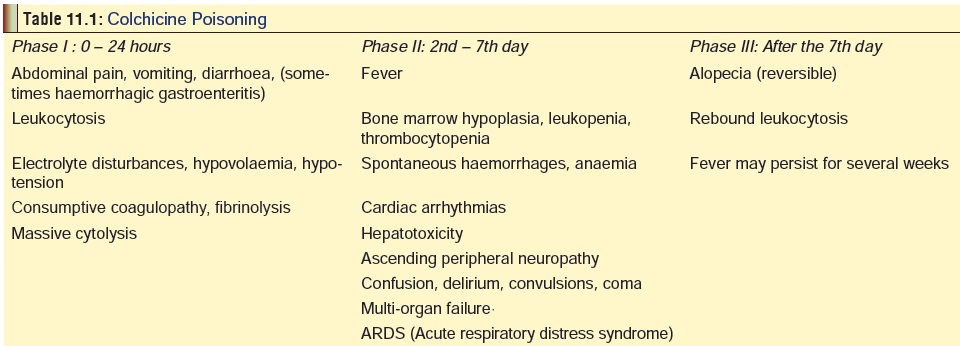
Clinical Features
Listed
in Table 11.1
Poisoning resulting from plant part
ingestion is usually less severe than the pure alkaloid (colchicine) poisoning.
Common manifestations after plant ingestion include nausea, vomiting,
diarrhoea, abdominal pain, tachycardia, and chest pain. Hypotension, bradycardia,
seizures, bone marrow suppression, coagulopathy, ECG changes, and death occur
rarely.
Usual Fatal Dose
·
1 gram of the fresh corm.
·
7 to 60 mg of colchicine (0.5 mg/kg
may be fatal).
Treatment
·
The following must be monitored:
o Fluid
and electrolyte balance.
o Renal
and liver function tests.
o Complete
blood count (CBC) with differential and platelet count (daily in symptomatic
patients).
·
All patients should be observed for
at least 12 hours, because of occasional late onset of manifestations.
· Colchicine is believed to undergo
enterohepatic recirculation.
·
Multiple dose activated charcoal may
be beneficial because it interrupts enterohepatic recirculation, and should
always be considered in patients with potentially serious or lethal ingestions.
·
Fluid and electrolyte status,
especially potassium levels, should be followed closely, with administration of
appropriate intra-venous fluids for replacement.
·
Central nervous symptoms and
ascending paralysis with respiratory involvement require aggressive supportive
care including mechanical ventilation.
·
Patients suffering from bone marrow
depression should be isolated to protect the patient from infection.
·
Granulocyte colony-stimulating
factor, 300 mg/day, IV, helps in normalising leukocyte count.
· Antidote: Specific goat colchicine Fab fragments adminis-tered as an infusion (400 to 500 mg). There are case reports of dramatic recovery from potentially lethal colchicine poisoning.
·
Haemodialysis and exchange transfusion
are not likely to be helpful because of the large apparent volume of
distribution of colchicine.
Autopsy Features
·
Multiple petechiae and ecchymoses
over visceral pleura, pericardium, and peritoneum.
·
Haemorrhagic oedema and congestion
of lungs.
·
Inflammation of stomach and
intestines.
· Fatty degeneration of liver.
Microscopy may reveal fatty changes and necrosis in the central portions of
hepatic lobules with cells demonstrating “colchicine bodies”, i.e. nuclei
containing clumps of chromatin material. In a recently reported case, autopsy
revealed hepatosplenomegaly (with significant haemorrhagic necrosis around
central hepatic veins) and acute tubular necrosis. Hepatocytes showed hydropic
or microvesicular fatty change, and portal triads were infiltrated by
mononuclei. In addition, left cardiac ventricle hypertrophy and cerebral oedema
were observed.
· Kidneys may demonstrate evidence of
acute tubular necrosis.
· Microscopy of bone marrow tissue: hypocellular marrowwith marked
depletion of erythropoietic and granulopoietic cells, and moderate depletion of
megakaryocytes.
Related Topics