Chapter: Clinical Cases in Anesthesia : Carcinoid Syndrome
What are the major anesthetic concerns in patients with carcinoid syndrome?
What are
the major anesthetic concerns in patients with carcinoid syndrome?
Although carcinoid tumors are relatively rare,
patients with this disease frequently have concurrent medical problems. Thirty
percent have carcinoid heart disease. The cause is unclear. Right-sided fibrous
plaque deposited on the tricuspid valve and right ventricular walls is the most
common finding. Tricuspid regurgitation is the most com-mon valvulopathy
associated with carcinoid tumors. If the pulmonary valve is involved, stenosis
rather than regurgi-tation is more prevalent. Carcinoid plaques are rarely
found on the left side of the heart, but do occur.
Anesthetic concerns include right-sided heart
failure and pulmonary hypertension. It is important to avoid increases in
pulmonary vascular resistance to prevent hypoxemia. High-dose nitrous oxide may
predispose to pulmonary hypertension. Patients with significant tricuspid
regurgita-tion should be kept well hydrated and tachycardia should be avoided.
These patients are more susceptible to supraven-tricular dysrhythmias as well.
Endocarditis prophylaxis should be undertaken with a penicillin or variant, and
under some circumstances an aminoglycoside. Treatment of hypotension with
catecholamines may produce worse physiologic problems. Catecholamines stimulate
secretion of substances from carcinoid tumors. Among these sub-stances are
mediators that produce hypotension and other components of the carcinoid
syndrome. Consequently treat-ment of hypotension with catecholamines can
produce a paradoxical exacerbation of hypotension.
Gastric carcinoid generally releases histamine,
thus bronchospasm can occur, which does not respond well to β-agonists or aminophylline. It is prudent to avoid drugs which release histamine such as d-tubocurarine, atracurium,
mivacurium, and morphine.
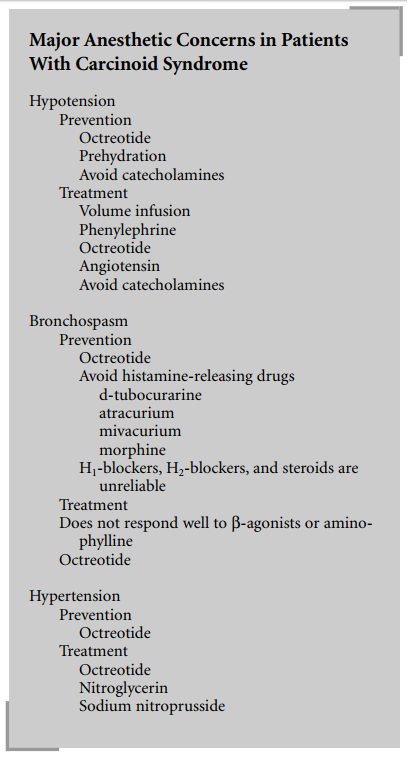
H1-blockers, H2-blockers, and steroids have been used prophylactically to
avoid severe reactions, but are unreliable. Succinylcholine should also be used
with caution, as abdominal wall fasciculations can increase intra-abdominal
pressure, thus squeezing the tumor causing further hormone release.
Pretreatment with a nondepolarizing neuromuscular blocker can decrease
fasciculations. If hypotension occurs intraoperatively it is important to give
volume and avoid the use of cate-cholamines or β-agonists. The use of angiotensin in a dose of
1.5 mg/kg may improve hypotension. Prehydration is of great benefit in these
patients as a generalized fluid deficit occurs due to secondary hormone release
from the tumor. Invasive monitoring to assess cardiovascular status is helpful
in some patients with cardiac disease, due either to carcinoid or intrinsic
myocardial disease itself. Acute intraoperative hypertension is often associated
with bron-chospasm, which is probably due to serotonin release. If hypertension
occurs acutely, the use of vasodilating agents, such as nitroglycerin or sodium
nitroprusside, is recom-mended.
Related Topics