Chapter: Modern Pharmacology with Clinical Applications: Drugs Used in the Treatment of Erectile Dysfunction
Individual Agents
INDIVIDUAL
AGENTS
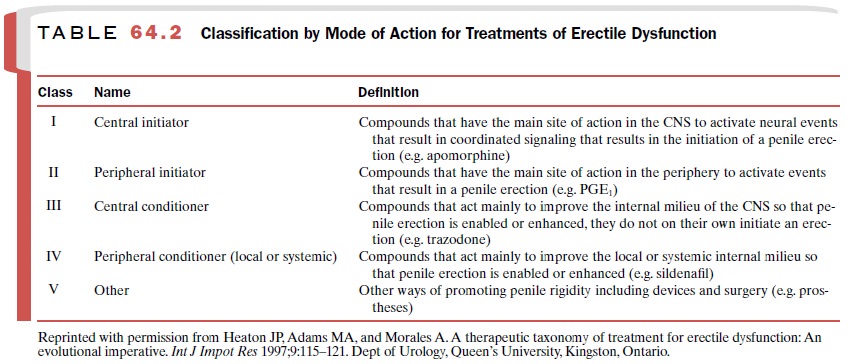
The pharmacological agents
useful in this disorder may be grouped under five broad categories of treatment
(Table 64.2). Such a classification system takes into ac-count the mode of drug
action, the route of administra-tion, and the means by which target organ
selectivity is achieved.
Oral medication for treatment of ED is relatively new. Earlier measures often employed the intracavernosal injection of a vasoactive agent or a systemic mode of drug administration.
Local injections or
dermal ap-plications were frequently required for satisfactory pharmacological
actions upon the vascular smooth mus-cles of the penis. Compounds with
relatively short dura-tion of action were found to be less than satisfactory in
maintaining penile erections.
Combinations of drugs have
sometimes been used to take advantage of the differing onset and duration of
action of the individual compounds. A rapid onset of ac-tion and a sufficient
duration are important characteris-tics of drugs used in the treatment of ED.
Vasoactive agents that are orally effective have been available for about 20
years, but sildenafil and apomorphine (buccal) have significantly improved upon
the therapeutic effi-cacy of orally active agents.
Alprostadil
Alprostadil (prostaglandin E1
[PGE1]; Edex, Topiglan)
exerts a number of effects, including systemic vasodila-tion, inhibition of
platelet aggregation, and stimulation of intestinal motility. PGE1
relaxes isolated smooth muscle cells contracted by norepinephrine. It has
be-come widely used in the treatment of ED. Alprostadil binds with PGE receptors
and results in a cyclic adeno-sine monophosphate (cAMP) mediated smooth muscle
relaxation. Little is known about the pharmacokinetics of PGE1, but
it is believed that as much as 80% is me-tabolized in one pass through the
lungs. Such rapid degradation probably accounts for its lack of significant
cardiovascular side effects when administered intracav-ernosally. PGE1
can also be metabolized in the penis.
PGE1 is not orally
effective. Its therapeutic success depends on its being injected intracavernosally
or ad-ministered transurethrally or intraurethrally. PGE1 has also
been used in combination with other agents, such as papaverine. The injection
does not appear to produce any long-term side effects on penile smooth muscle.
Transurethral therapy with alprostadil, such as MUSE (alprostadil urethral
suppository or medicated urethral system for erection) is
also an effective therapeutic technique,
and there may be a role for this form of ad-ministration in selected patients
with ED. The intracav-ernosal injection of alprostadil (e.g., alprostadil
alfadex; Edex, Viridal) is safe and
effective in patients with ED when
sildenafil is ineffective. Both of these delivery sys-tems have been used in
the treatment of ED. MUSE can also be used in conjunction with a penile
constrictor de-vice (e.g., ACTIS).
Apomorphine
Apomorphine (Uprima) is a short-acting central and pe-ripheral
dopamine receptor agonist that can elicit male sexual responses. Dopamine
appears to have an impor-tant role in normal erectile function. Apomorphine is
a D1-like, D2-like dopamine receptor agonist.Apomorphine
is not a new drug, and it has been used with limited suc-cess in ameliorating
the symptoms of Parkinson’s disease and to induce emesis. It is not orally
active except for a special buccal formulation, but it can be given
parenter-ally, usually subcutaneously. Apomorphine is rapidly cleared from the
kidney because of its high lipid solubility, its large volume of distribution,
and its rapid metabolism.
Aside from sildenafil,
apomorphine is one of the few orally active (buccal route) pharmacological
agents used in the treatment of ED. Apomorphine stimulates penile erection in
both normal men and in men who are impotent. Apomorphine can be the drug of
choice in patients with coexisting benign prostatic hyperplasia (BPH), coronary
artery disease, and hypertension.
When formulated into a
controlled release sublin-gual capsule, apomorphine becomes a very effective
orally active drug representative of a new class of cen-trally acting drugs
useful in the treatment of ED. It has a narrow range (2 to 6 mg) of effective
doses for its erectogenic actions, with the higher doses being more effective
in inducing erections. Apomorphine can cause nausea, emesis, drowsiness, and
dizziness.
Androgens: Testosterone
Androgen deficiency can lead
to decreases in nocturnal erections and libido. Hypogonadism is associated with
impotence, yet erection in response to visual stimula-tion is preserved in men
with hypogonadism, suggesting that androgens are not essential for erection.
Although androgens can enhance male sexual function, testos-terone therapy for
the treatment of ED should be dis-couraged unless the cause is clearly related
to hypogo-nadism. Androgen therapy in normal men may enhance sexual behavior
but is without significant effect upon erectile function.
Usefulness of oral
methyltestosterone is limited in men with hypogonadal impotence. Improvement
follow-ing transdermal testosterone may require several months of therapy.
Androgen replacement regimens for treating male hypogonadism include
long-acting intramuscular injections (e.g., testosterone enanate, testosterone
cypi-onate) and oral preparations (e.g. methyltestosterone, fluoxymesterone).
Transdermal patches (Testoderm, Androderm) and topical testosterone gel
(Androgel) are also available. Transdermal testosterone also may im-prove sexual
function and psychological well-being in women who have undergone oophorectomy
and hys-terectomy. Transdermal delivery systems can provide a more constant
serum testosterone level than do intra-muscular injections, but they are more
expensive.
Papaverine
Papaverine (Pavabid) is a nonspecific
phosphodi-esterase inhibitor that increases cAMP and cGMP lev-els in penile
erectile tissue. Papaverine is particularly known as a smooth muscle relaxant
and vasodilator. Its principal pharmacological action is as a nonspecific va-sodilator
of smooth muscles of the arterioles and capil-laries. Various vascular beds and
smooth muscle re-spond differently to papaverine administration both in
intensity and duration. Papaverine decreases the resist-ance to arterial inflow
and increases the resistance to venous outflow.
Papaverine is highly
effective in men with psy-chogenic and neurogenic ED but less effective in men
with vasculogenic ED. Papaverine–phentolamine com-binations have been used in
self-injection procedures. Papaverine doses may range from 15 to 60 mg.
Papa-verine treatment in patients with severe arterial or ve-nous incompetence
is usually unsuccessful, but autoin-jections using low doses sufficient to
achieve an erection are safe and efficient.
Major side effects associated
with papaverine ther-apy include priapism, corporeal fibrosis, and occasional
increases in serum aminotransferases. Intracorporeal scarring may be related to
the low pH of the vehicle that is necessary to solubilize papaverine. Attempts
to buffer papaverine to render it more suitable for intracaver-nosal injection
have not been entirely satisfactory, and such delivery may still lead to
intracorporeal scarring.
Phentolamine
Human erectile tissue has a
population of membrane receptors that are predominantly of the α-adrenoceptor subtype.
Phentolamine (Vasomax) is a
nonselective α- adrenoceptor blocking agent , and like other such agents, it has
been used to treat ED. Nonselective adrenoceptor antagonists may provoke a
reflex that increases both sympathetic outflow and the release of
norepinephrine.
Phentolamine has been used
orally and intracaver-nosally in the treatment of ED. Following oral
adminis-tration, phentolamine has a plasma half-life of about 30 minutes and a
duration of action of 2 to 4 hours. An in-tracavernosal injection of
phentolamine results in the drug reaching maximum serum levels in about 20 to
30 minutes. It is rapidly metabolized.
Phentolamine has been used in
combination with papaverine, chlorpromazine, and vasoactive peptides in the
treatment of ED.
Side effects of phentolamine
are dose related. It may cause orthostatic hypotension, reflex tachycardia,
cardiac arrhythmias, and rarely, myocardial infarction. Phentolamine also may
reduce sperm motility in vitro.
Other α-adrenoceptor receptor
antagonists include yohimbine, phenoxybenzamine, and thymoxamine. Yo-himbine is
an α2-adrenoceptor antagonist, and
thymox-amine is a competitive and relatively selective blocking agent for α1- adrenoceptors.
Phenoxybenzamine blocks both α1- and α2-adrenoreceptors, although it has a greater affinity for the α1-subtype. All three of these β
-receptor blocking drugs can induce penile erection, but their ef-fects are
generally less consistent and less effective than those of phentolamine. Yohimbine
is only moderately ef-fective in treating patients with organic impotence, and
side effects may include postural hypotension, heart pal-pitations, fine
tremors, and cavernosal fibrosis, especially following intracavernosal
injections.
Sildenafil
Sildenafil (Viagra) was developed more than 10 years
ago as an antihypertensive and antianginal drug. It proved ineffective in these
applications but was shown to affect the smooth muscles of the penis.
Sildenafil is a selective
inhibitor of cGMP-specific PD-5 and therefore inhibits the degradation of cGMP.
PD-5, the predominant type in the corpus cavernosum, also is present in other
tissues (e.g., lungs, platelets, and eye). The selective inhibition of this
enzyme facilitates the release of nitric oxide and smooth muscle relaxation of
the corpus cavernosa. Sildenafil enhances erection by augmenting nitric
oxide–mediated relaxation pathways. It has been suggested that sildenafil’s
mechanism of action is due to cross-talk between cGMP- and cAMP-dependent transduction
pathways within the cavernous muscles.
Sildenafil is readily
absorbed after oral administra-tion and reaches peak plasma levels after about
an hour. It undergoes hepatic metabolism and has a termi-nal half-life of about
4 hours. An initial dose of 50 mg is taken about an hour prior to sexual
activity to induce penile erection.
Orally administered
sildenafil is an effective and well-tolerated treatment for men with ED,
including those with diabetes mellitus. It has also been used for so-called salvage
therapy in men who do not respond to intracorporeal injections of other agents.
Headache is a common side
effect, as are flushing and rhinitis. More serious side effects include
definite or suspected myocardial infarctions and cardiac arrest.
Trazodone
Trazodone (Apothecon) is also classified as an
antide-pressant agent. It is a selective serotonin reuptake in-hibitor (SSRI),
partial agonist at postsynaptic 5-HT1A receptors, and exhibits α-adrenoceptor blocking
ac-tions.
Trazodone may cause priapism
and enhance libido, and it prolongs nocturnal erections. This drug has been
used both orally and by intracavernosal injection. It can be used alone or in
combination with yohimbine. Overall, trazodone has not been as effective in
treating ED as other available agents. However, it may be an op-tion for
selected patients, particularly those with per-formance anxiety or low libido.
Other Agents
Many other drugs and herbals
exhibit varying degrees of potency with respect to penile erection. Some have undergone
limited clinical trials, while others are asso-ciated with anecdotal reports.
Generally, these agents are not particularly effective and are not widely used
among mainstream therapeutic options for ED.
Linsidomine (SIN-1) is an
active metabolite of the antianginal drug molsidomine. Its mechanism of action
upon the corpus cavernosum involves the release of ni- tric oxide. Injected
intracavernosally it can produce pe-nile erections, but its clinical usefulness
has not been fully established.
Nitroglycerin (also
isosorbide nitrate) relaxes iso-lated strips of human corpus cavernosum. Its
mecha-nism involves the stimulation of guanylate cyclase. Clinically,
nitroglycerin has been of limited use in the treatment of ED.
Minoxidil, an
antihypertensive agent, produces arte-riolar vasodilation by an unknown
mechanism. In lim-ited clinical studies, minoxidil increases penile rigidity
and has been used in the long-term treatment of organic impotence.
Naltrexone, an orally active
opioid receptor antago-nist, restores erectile function in some patients with
id-iopathic ED.
Calcitonin gene–related
peptide (CGRP) induces a dose-related increase in penile arterial inflow,
cav-ernous smooth muscle relaxation, cavernous outflow occlusion, and an
erectile response. CGRP plus PGE1 may be an alternative to penile
implants in selected pa-tients.
Forskolin, an herbal, relaxes
smooth muscle. In-jected intracavernosally, forskolin has been of limited use
in the treatment of vasculogenic impotence.
Other herbal remedies or
so-called natural products purportedly can enhance male sexual activity. Some
may contain yohimbine. Natural prosexual agents of herbal origin include Epidemicum sagthatum, Tribulas terrestris, and Murira puama. Their use in folk medicine in China and other countries is likely due to their sexual
stimulating properties and their aphrodisiac effects. Ginkgo biloba extract also has been used in the therapy of ED and sexual dysfunction.
Drug Interactions
Orally active agents used in
the treatment of ED are more affected by aging and disease processes than are
those injected intracavernosally. In addition, alterations in hepatic
metabolism and/or renal clearance in the eld-erly man influence the frequency of ap-pearance of
adverse reactions between several coad-ministered drugs in the treatment of ED.
For example, the concomitant use of sildenafil and nitroglycerin is
contraindicated by cardiovascular complications. Also, the use of testosterone
in the presence of androgen-dependent tumors may promote tumor growth.
Sildenafil has other minor
adverse effects, such as headache, nasal congestion, and flushing. There are no
clinically significant drug interactions between sildenafil and apomorphine.
Apomorphine, like sildenafil, is orally active. However, unlike sildenafil, it
exerts its ac-tion through the central nervous system. Apomorphine can produce
dizziness, nausea, pallor, and hypotension, and in the presence of ethanol, it
purportedly increases the incidence of these side effects. Such a synergy
caused by ethanol and apomorphine coadministration is not unique and would
likely be present with other agents that induce mild hypotension.
The concomitant intake of
grapefruit juice increases the concentration of many drugs (e.g., testosterone,
sildenafil) in humans. Such actions appear to be medi-ated mainly by the
suppression of the cytochrome P450 enzyme CYP3A4 in the small intestine. The
resultant di-minished first-pass metabolism and increased bioavail-ability can
lead to increased drug levels in the blood. Because sildenafil is metabolized
by CYP3A and to a lesser extent by CYP2C9, grapefruit juice can reduce the
clearance of this drug. Other drugs can either in-crease or decrease serum
levels of sildenafil. Admin-istration of cimetidine, erythromycin, or ritonavir
can lead to increases in serum concentrations of sildenafil, while rifampin
diminishes blood levels of sildenafil.
Therapy with phentolamine may
result in reflex tachycardia, arrhythmias, and hypotension; the latter ef-fect
can be exacerbated by other vasodilatory drugs and by the simultaneous
ingestion of ethanol. The pharma-cological actions of trazodone can be reduced
by parox-etine and possibly other SSRIs.
Related Topics