Chapter: Microbiology and Immunology: Immune Response
Humoral Immunity
Humoral Immunity
Humoral immunity is based on the action of antibodies and complement. It is directed primarily against:
· Extracellular bacteria, in particular exotoxin-producing bacteria, such as Corynebacterium diphtheriae, Clostridium tetani, etc.,
· Bacteria whose virulence is due to polysaccharide capsules (e.g., Haemophilus influenzae, Neisseria meningitidis,Streptococcuspneumoniae, etc.), and
· Certain viruses that cause infection through respiratory or intestinal tract. The humoral immunity also participates in the pathogenesis of hypersensitivity reactions and certain autoimmune diseases.
Production of antibodies is the main feature of humoral immune responses. The production of antibodies follows a characteristic pattern as follows:
a) Lag phase: This is the immediate phase following exposure toantigen. During this phase, no antibodies are detected in circulation.
b) Log phase: This is the next phase characterized by a steadyrise in antibody titers in the circulation.
c) Plateau: This is a phase of equilibrium between antibodysynthesis and catabolism.
d) Phase of decline: This phase is characterized by an increasein the catabolism of antibodies compared to the production of antibodies, leading to a fall in antibody titer in the circula-tion. Humoral immune response is of two types: primary and secondary.
Primary Response
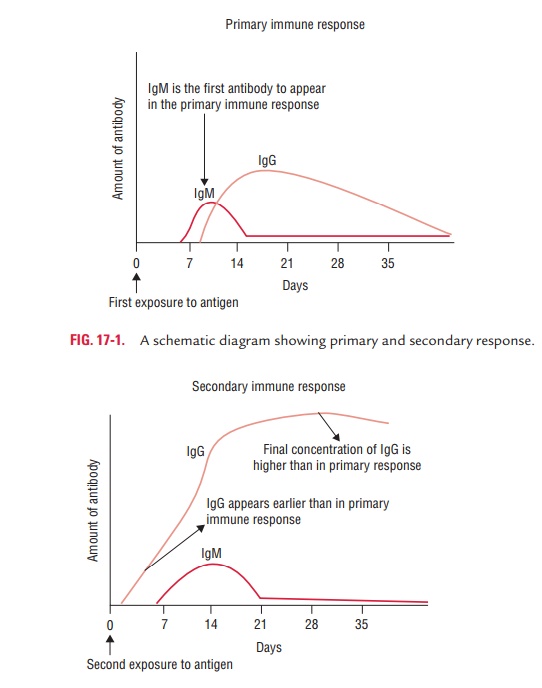
During the primary response, when an individual encounters an antigen for the first time, antibody response to that antigen is detectable in the serum after a longer lag period than occurs in the secondary response. The serum antibody concentration continues to rise for several weeks and then declines; it may drop to very low levels. During this primary response, a small clone of B cells and plasma cells specific for the antigen are formed.
The lag period is typically of 7–10 days duration but can be longer, even for weeks, depending on the nature of the anti-gen. For example, the lag phase may be as long as 2–3 weeks with some antigens, such as diphtheria toxoid, while it may be a short as a few hours with pneumococcal polysaccharide. The lag period also depends on dose of the antigen and the route of administration whether oral or parenteral.
IgM is the first antibody to be formed, followed by IgG, IgA, or both. IgM levels tend to decline sooner as compared to IgG levels (Fig. 17-1).
Secondary Response
The antibody response is typically more rapid in the second-ary response, due to second encounter with the same antigen, or a closely related “cross-reacting” antigen, months or years after the primary response. The lag period is typically very short (only 3–5 days). The level of antibody is also much higher than that during the primary response.
These changes in secondary response are attributed to the persistence of antigen-specific “memory cells” following the first contact with the antigen. These memory cells proliferate in large numbers to produce large clones of specific B cells and plasma cells that mediate the secondary response. In the secondary response:
· The amount of IgM produced is qualitatively similar to that produced after the first contact with the antigen; however, much more IgG is produced and the level of IgG tends to persist much longer than in the primary response.
· Furthermore, such antibody tends to bind antigen more firmly (i.e., to have higher affinity) and thus to dissociate less easily. Improved antibody binding is due to mutations that occur in the DNA that encodes the antigen-binding site. This process is calledsomatic hypermutation.
Fate of Antigen in Tissues
Route of administration of antigen affects the site of localiza-tion of these antigens in the body. For example, most of the antigens introduced subcutaneously are localized mainly in the draining lymph nodes and only a small amount is there in the spleen. On the other hand, most of the antigens introduced intravenously are localized in the spleen, liver, bone marrow, kidney, and lungs but not in lymph nodes. Approximately, three-fourths of these antigens are broken down by reticuloepi-thelial cells and are excreted out in the urine.
Related Topics