Chapter: Clinical Pharmacology: Fundamentals of clinical pharmacology
Pharmacodynamics
Pharmacodynamics
Pharmacodynamics is the study of the drug
mechanisms that pro-duce biochemical or physiologic changes in the body. The
inter-action at the cellular level between a drug and cellular compo-nents,
such as the complex proteins that make up the cell mem-brane, enzymes, or
target receptors, represents drug action. The response resulting from this drug
action is the drug effect.
It’s the cell that matters
A drug can modify cell function or rate of
function, but it can’t impart a new function to a cell or to target tissue.
Therefore, the drug effect depends on what the cell is capable of
accomplish-ing.
A drug can alter the target cell’s function by:
·
modifying the cell’s physical or chemical environment
·
interacting with a receptor (a specialized location on a cell membrane
or inside a cell).
Agonist drugs
Many drugs work by stimulating or blocking drug
receptors. A drug attracted to a receptor displays an affinity for that
receptor. When a drug displays an affinity for a receptor and stimulates it,
the drug acts as an agonist. An
agonist binds to the receptor and produces a response. This ability to initiate
a response after bind-ing with the receptor is referred to as intrinsic activity.
Antagonist drugs
If a drug has an affinity for a receptor but
displays little or no in-trinsic activity, it’s called an antagonist. An antagonist prevents a response from occurring.
Reversible or irreversible
Antagonists can be competitive or noncompetitive.
·
A competitive antagonist
competes with the agonist for recep-tor sites. Because this type of antagonist
binds reversibly to the re-ceptor site, administering larger doses of an
agonist can overcome the antagonist’s effects.
·
A noncompetitive antagonist
binds to receptor sites and blocks the effects of the agonist. Administering
larger doses of the ago-nist can’t reverse the antagonist’s action.
Regarding receptors
If a drug acts on a variety of receptors, it’s said
to be nonselective and can cause multiple and widespread effects. In addition,
some receptors are classified further by their specific effects. For exam-ple,
beta receptors typically produce increased heart rate and bronchial relaxation
as well as other systemic effects.
Beta receptors, however, can be further divided
into beta1 re-ceptors (which act primarily on the
heart) and beta2 receptors (which act primarily on smooth
muscles and gland cells).
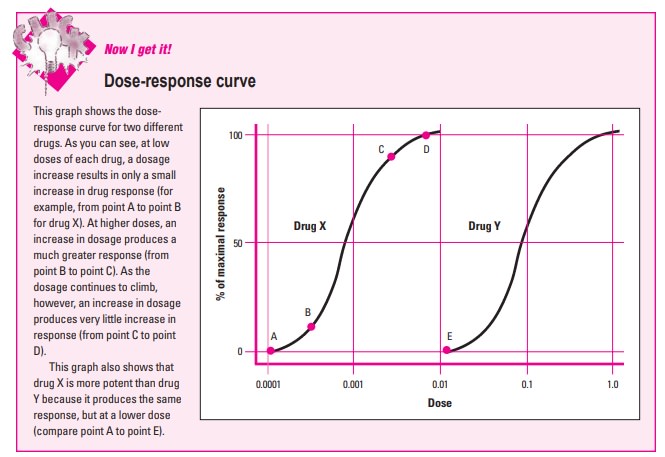
Potent power
Drug potency refers to the relative amount of a
drug required to produce a desired response. Drug potency is also used to
compare two drugs. If drug X produces the same response as drug Y but at a
lower dose, then drug X is more potent than drug Y.
As its name implies, a dose-response curve is used
to graphi-cally represent the relationship between the dose of a drug and the
response it produces. (See Dose-response
curve)
Maximum effect
On the dose-response curve, a low dose usually
corresponds to a low response. At a low dose, a dosage increase produces only a
slight increase in response. With further dosage increases, the drug response
rises markedly. After a certain point, however, an increase in dose yields
little or no increase in response. At this point, the drug is said to have reached
maximum effectiveness.
Margin of safety
Most drugs produce multiple effects. The
relationship between a drug’s desired therapeutic effects and its adverse
effects is called the drug’s therapeutic
index. It’s also referred to as its margin
of safety.
The therapeutic index usually measures the
differ-ence between:
·
an effective dose for 50% of the patients treated
·
the minimal dose at which adverse reactions occur.
Narrow index = potential danger
Drugs with a narrow, or low, therapeutic index have
a narrow margin of safety. This means that there’s a nar-row range of safety
between an effective dose and a lethal one. On the other hand, a drug with a
high thera-peutic index has a wide margin of safety and poses less risk of
toxic effects.
Related Topics