Chapter: Pathology: Breast Pathology
Malignant Neoplasms
MALIGNANT NEOPLASMS
Carcinoma of the breast is the most common cancer in
women and affects 1 in 9 women in the United States.
It is also the second most common cause of cancer death. The incidence is
increasing and is higher in the United States than in Japan. Many risk factors
have been identified.
The incidence increases with
the following factors:
•
Age
•
Unusually long/intense exposure to estrogens (long length of
reproductive life, nulliparity, obesity, exogenous estrogens)
•
Presence of proliferative fibrocystic changes, especially atypical hyperplasia
•
First-degree relative with breast cancer
Hereditary influences are
thought to be involved in 5–10% of
breast cancers, with important genes as follows:
•
BRCA1 (error-free repair of DNA double-strand breaks) chromosome 17q21
•
BRCA2 (error-free repair of DNA double-strand breaks) chromosome 13q12.3
•
TP53 germline mutation (Li-Fraumeni syndrome)
Carcinoma in situ and risk of invasive carcinoma. About 35% of women with untreated DCIS will develop invasive
cancer, usually in the same quadrant of the breast. About 35% of women with
LCIS will develop invasive lobular or ductal car-cinoma, in either breast.
Breast cancer is most common
in the upper outer quadrant. Gross examination of a breast cancer typically
shows a stellate, white-tan, gritty mass. Clinically, it can cause:
•
Mammographic calcifications or architectural distortion
•
Palpable solitary painless mass
•
Nipple retraction or skin dimpling
•
Fixation of breast tissue to the chest wall
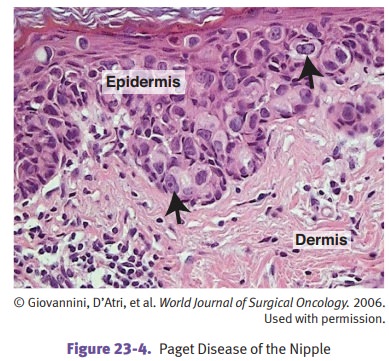
Paget disease of the nipple is an
intra-epidermal spread of tumor cells from an underlying ductal carcinoma
in situ or invasive ductal carcinoma. The tumor cells often lie in lacunae, and
there can be a dermal lymphocytic infiltrate.
Histologic variants of breast
cancer are as follows:
•
Preinvasive
lesions include ductal carcinoma in situ (DCIS) and lobular carci-noma in situ (LCIS). Preservation of the myoepithelial cell layer distinguishes
them from their invasive counterparts.
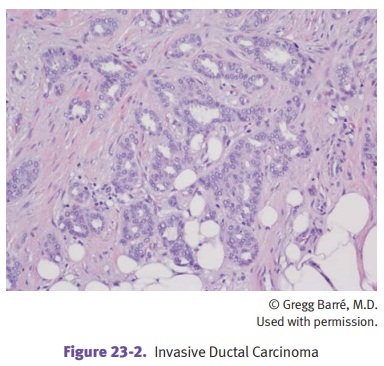
•
Invasive (infiltrating) ductal carcinoma is the most common form
(>80% of cases). Microscopically, it shows tumor cells
forming ducts within a desmoplas-tic stroma. About 70% of cases are ER/PR
positive and 30% overexpress HER2
•
Invasive
(infiltrating) lobular carcinoma (5–10% of cases) is characterized by small, bland tumor cells forming a single-file
pattern.
•
Multifocal and bilateral disease occurs commonly.
°°
About 50% are ER/PR-positive; these tumors do not overexpress HER2.
•
Mucinous
(colloid) carcinoma is characterized microscopically by clusters of bland tumor cells floating within pools of
mucin. It has a better prognosis.
°°
Hormone receptors are positive; these tumors do not overexpress
HER2.
•
Tubular
carcinoma rarely metastasizes and has an excellent prognosis.
°°
Hormone receptors are positive; these tumors do not overexpress
HER2.
•
Medullary
carcinoma is characterized microscopically by pleomorphic tumor cells forming syncytial groups surrounded by a dense
lymphocytic host response. It has a better prognosis.
Hormone receptors are negative;
the tumors do not overexpress HER2.
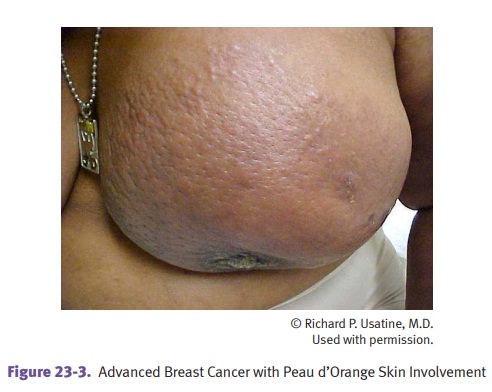
•
Inflammatory carcinoma is related to tumor invasion into the dermal
lymphat-ics with resulting lymphatic edema; it presents with red, warm,
edematous skin. The prognosis is poor.
The term peau d’orange is used
when the thickened skin resembles an orange peel. This is caused by the
accentuation of the attachments of the suspensory ligaments of Cooper to the
dermis.
Mammary Paget disease (Paget disease of the nipple) is
commonly associated with an underlying invasive
or in situ ductal carcinoma. It may present with ulceration, ooz-ing, crusting,
and fissuring of the nipple and areola. Microscopic examination shows
intraepidermal spread of tumor cells (Paget cells), with the cells occurring
singly or in groups within the epidermis; there is often a clear halo surrounding
the nucleus.
The prognosis of
breast cancer depends on the following:
•
Axillary lymph node status as determined by sentinel node biopsy
(SNB) or axillary dissection. In most cases, SNB is recommended to evaluate
clinically tumor-free regional nodes.
•
Size of tumor
•
Histological type and grade of tumor
•
ER/PR receptor status is used to select patients for endocrine
forms of therapy.
•
Overexpression of HER2/neu is associated with more aggressive
behavior than other types of breast cancer; patients may respond to therapy
with trastu-zumab.
Treatment of breast cancer
depends on the stage and other tests.
•
Urokinase plasminogen activator (uPA) and plasminogen activator
inhibitor (PAI-1) as measured by ELISA are used to guide treatment decisions
with node-negative breast cancer, along with multiparameter gene expression
analysis.
•
Cancer antigen 15-3 (CA 15-3), cancer antigen 27.29 (CA 27.29), and
carcino-embryonic antigen (CEA) are used to monitor patients with metastatic
disease undergoing therapy.
Although the majority of
cancers in the breast are primaries, cancer
from other organs can spread to the
breast. Lung cancer may spread by contiguity or via the lymphatics.