Chapter: Clinical Cases in Anesthesia : Kidney Transplantation
Discuss the treatment of hyperkalemia and its associated metabolic problems
Discuss
the treatment of hyperkalemia and its associated metabolic problems.
Patients with chronic renal failure experience
an extraor-dinarily wide range of serum K+ levels ranging from 2.5
to 6.0 mEq/L. Acute hyperkalemia suppresses electrical con-duction and can
ultimately cause cardiac arrest. Associated ECG changes include prolonged PR
intervals, widened QRS complexes, and peaked T waves before ventricular
fibrilla-tion actually occurs. Fatal dysrhythmias may occur without these gradual
changes.
Extracellular acidosis results in an increased
concentra-tion of hydrogen ion (H+), which moves into the cell along
its concentration gradient. To preserve electrical neutrality, K+
moves out of the cell. In this way, extracellular acidosis promotes
extracellular hyperkalemia. In acute metabolic acidosis, serum K+
increases approximately 0.5–0.8 mEq/L for every drop in pH of 0.1 units.
Normally the ratio of intracellular to extracellular K+
concentration is approxi-mately 40:1 or 160:4 mEq/L in vivo. This is maintained
by an energy-dependent Na+–K+-ATPase pump at the cell
membrane, which brings K+ intracellularly against its concentration
gradient.
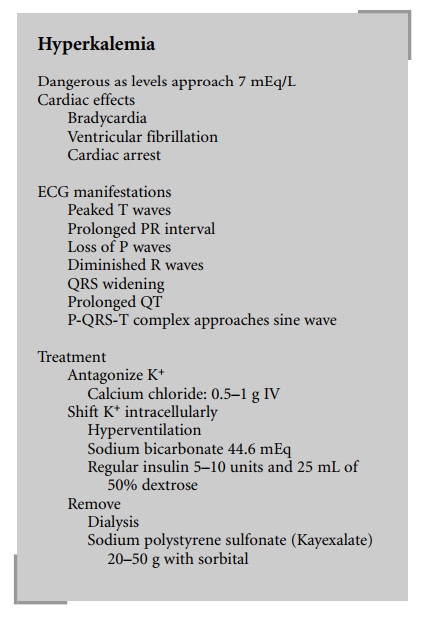
In chronic renal failure patients, aggressive
treatment of hyperkalemia is appropriate. The treatment for acute hyperkalemia
consists of the intravenous administration of insulin 5–10 units with 25 mL of
50% dextrose, sodium bicarbonate 44.6 mEq/L, and calcium chloride 500 mg.
Insulin promotes transmembrane cellular transport of K+ intracellularly,
thus reducing serum levels of K+. Calcium chloride is given to
reduce the arrhythmogenic potential.
Related Topics