Chapter: Surgical Pathology Dissection : Maxilla
Surgical Pathology Dissection : Maxilla
Maxilla
Resections
of tumors involving the passages of the nose and paranasal sinuses present the
ulti-mate challenge in surgical pathology dissection. These passages are walled
by bony structures that defy efforts to section, expose, and sample. Moreover,
the three-dimensional anatomy of these regions is inherently complex and
difficult to reconstruct once the specimen has been removed from the patient.
Nowhere are these difficulties more significantly encountered than during
re-section of the maxilla.
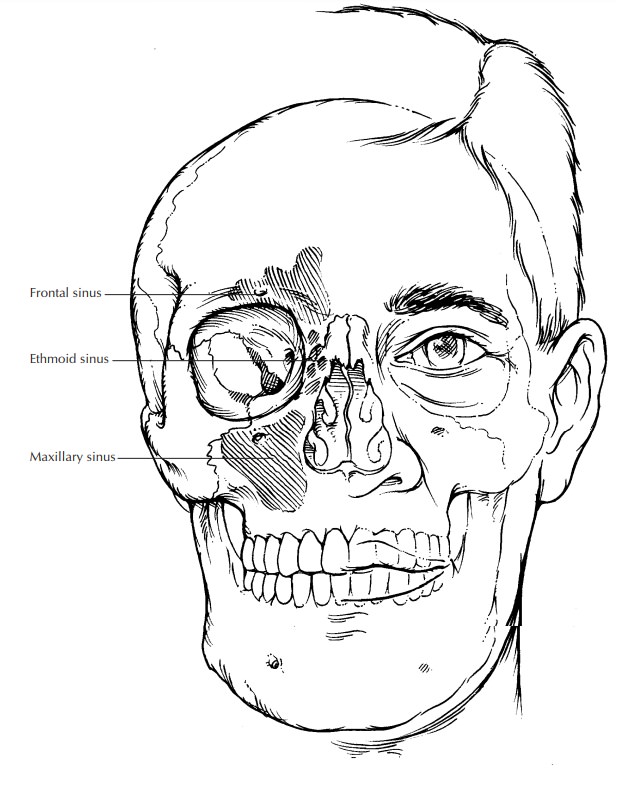
The
maxillary sinus is somewhat pyramidal in shape and is surrounded on all sides
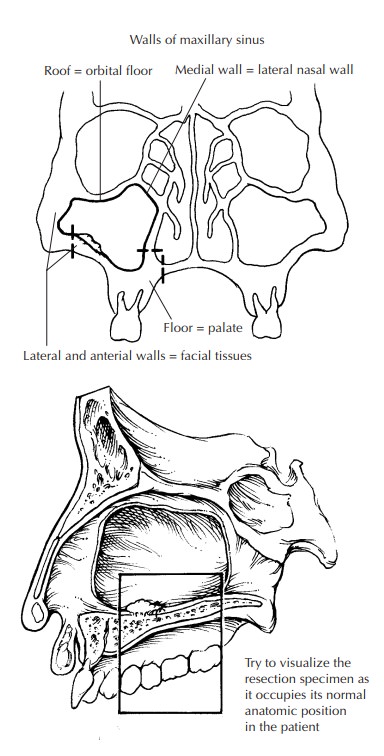
by cranio-facial bone. The daunting anatomic complexity of this region can be
simplified by envisioning yourself in a room with a floor, a ceiling, and four
walls. At your feet is the hard palate. Pass through this floor, and you enter
the oral cavity. Above your head is a ceiling that forms the floor of the
orbit. Pass through this ceiling, and you enter the orbital cavity. Turn
medially, and you face a wall that is shared with the nasal cavity (i.e., the
lateral nasal wall). Pass through this wall, and you enter the nasal chamber.
The remaining walls are not shared with other chambers. In-stead, the anterior
and lateral walls form the bony surfaces of the face, which are bounded by the
soft tissues and skin of the cheek. The posterior wall forms a boundary with
the musculature and bony processes of the pterygoid complex. This
concep-tualization should help you discern the specific location of a tumor in
the maxillary sinus and understand the paths of tumor spread into adja-cent
chambers and anatomic structures.
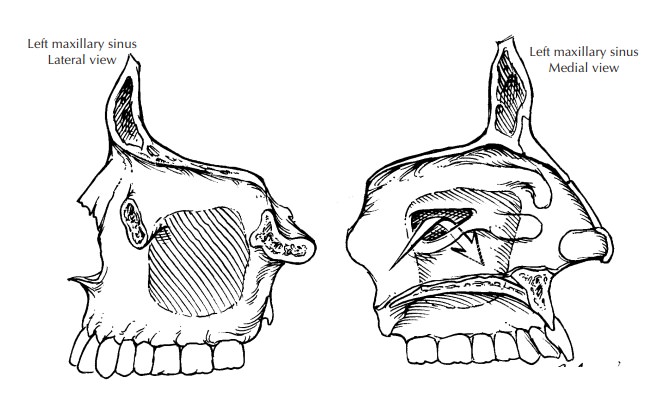
With
this image in mind, orient the maxillec-tomy specimen. Remember that only a
portion of the maxilla is generally removed during a cancer resection (i.e.,
partial maxillectomy). Con-sequently, only some of the surfaces are present,
leaving the sinus exposed to visual inspection. The extent of the resection
depends on the location and spread of the tumor. Specimen orientation is
greatly facilitated by the recognition of a few key landmarks. Teeth, when
present, identify the floor of the maxillary sinus (alveolar process) and help
you discern the anterior and lateral aspects of the maxilla. The nasal choana
are seen as smooth longitudinal folds or pouches of mucosa-lined tissues. These
form the lateral wall of the nasal sinus and identify the medial aspect of the
maxilla. Some specimens include the eye. In these cases, identification of the
superior and anterior aspects of the specimen is obvious. If present, skin from
the cheek marks the lateral and/or anterior aspect of the specimen. If you have
done your best to identify these landmarks but still have trouble with
orientation, do not hesitate to contact the surgeon.
Once you
have confidently oriented the speci-men, measure it in three dimensions.
Identify and describe the anatomic boundaries of the specimen and note the
presence of important anatomic structures (e.g., eye, skin, nasal choana,
teeth). Ink the external margins of the soft tissue envel-oping the maxilla,
being careful not to let ink seep into the sinus. Without sectioning the
specimen, look into the exposed maxillary sinus and try to identify the tumor.
In addition to documenting the size of the tumor, determine its location within
the maxillary sinus. Specifically, identify which walls are grossly involved by
tumor. De-termining the site of tumor origin helps guide further sectioning of
the specimen to determine the path of tumor spread. For instance, a tumor
arising from the floor of the sinus generally ex-tends inferiorly and laterally
into the palate and the alveolar process of the maxilla (infiltrating between
and around molar teeth). More medially placed tumors are prone to extend into
the nasal cavity. Tumors along the lateral wall may in-filtrate the skin and
soft tissues of the cheek. Tumors involving the roof of the sinus tend to
extend into the orbital cavity, ethmoid air cells, ethmoid sinus, or cribriform
plate. For tumors in-volving more than one chamber, try to determine the
epicenter of the tumor. For example, if a tumor involves the floor of the
maxillary sinus, try to distinguish between a maxillary sinus carcinoma that
extends inferiorly into the palate and an oral cavity carcinoma that extends
superiorly into the maxillary sinus.
Depending
on your laboratory’s preferences, the specimen can be dissected in the fresh
state or be sectioned after fixation in formalin. After tissue has been
obtained for special studies as needed, we recommend fixation before further
processing. Tissue fixation facilitates the difficult process of stripping
mucosal margins from un-derlying bone. Tissue fixation also minimizes tissue
fragmentation and distortion should sawing be required to section through bone.
Finally, adequate fixation is essential before the sample can be processed in
demineralizing solutions should specimen decalcification be required.
Begin
your dissection by sampling all of the margins including the soft tissues,
bone, mucosa, and skin. The number and type of margin sections depend on the
nature and extent of the resection. For example, if the medial wall of the
sinus is removed, you need to sample the mucosa all along the nasal cavity
margin. If the resection includes the orbit, you need to submit a shave section
of the optic nerve. Before taking these sec-tions, it is helpful first to
tabulate all of the various chambers and tissue components present in the
specimen so that no margin is overlooked. Sam-pling some of these margins can be
challenging. For example, the presence of teeth and underly-ing bone are
formidable barriers to well-oriented perpendicular sections that radiate from
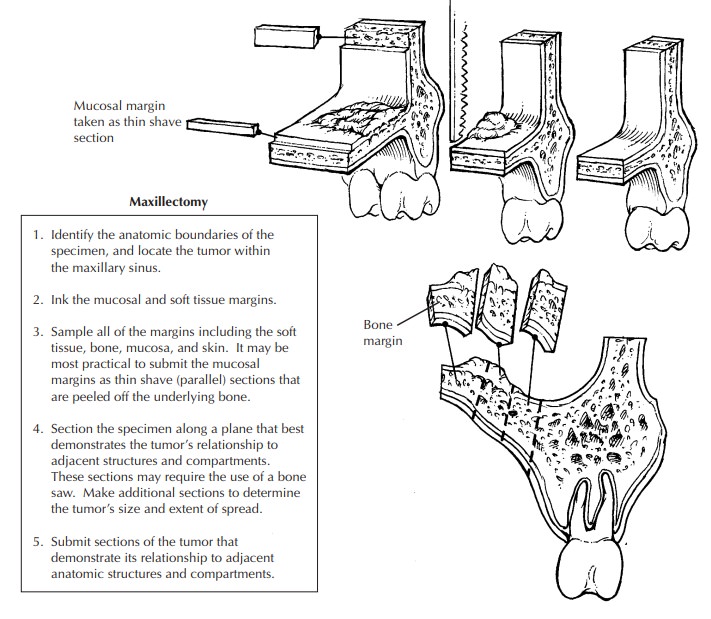
the edge of the specimen toward the center of the tumor. Instead of the
standard perpendicular sections, the mucosal edges of the maxillary resection
(par-ticularly along the alveolar process of the maxilla) may have to be taken
as thin parallel sections that are gently peeled off the underlying bone.
Again, these sections are easier to obtain if the mucosa is well fixed. The
soft tissue margins, in contrast, can be submitted as perpendicular sec-tions.
Be sure to include in your gross description details of the precise location
and type of each margin. A photograph that indicates the location of each margin
section is highly recommended.
After
all of the margins have been sampled, bisect the specimen along a plane that
passes through the epicenter of the tumor and best dem-onstrates the tumor’s
relationship to adjacent compartments. Before making this first cut, it may be
useful to consult the preoperative imaging studies to determine the location of
the tumor and its path of spread. This section may require the use of a band
saw, particularly when the sections must pass through the dense bone of the
alveolar process and palatal alveolus. Teeth are particularly dense tissues,
and they are dif-ficult to section even with powerful bone saws. Unless there
are indications to sample a tooth, sections through the alveolar process of the
man-dible should avoid the teeth. Direct the blade of the saw between the
teeth. Make additional sections to further assess the extent of the tumor and
its relationship to surrounding structures. When intact teeth are included
within the portion of the specimen to be histologically evaluated, it may be
prudent to remove the crowns of these teeth. This practice shortens the
decalcification time and lessens decalcification-induced artifacts. Removal of
crowns can be facilitated by use of a bone saw or dental drill with a stream or
spray of coolant water.
Now that
the tumor has been more fully ex-posed, describe its appearance and growth
char-acteristics. Is the tumor exophytic, endophytic, erosive, and/or
infiltrative? Measure and record its dimensions including its deepest level of
in-vasion. Determine the anatomic structures and compartments the tumor
involves. Is the tumor confined to the maxillary sinus? If there is inva-sion
into bone, has the tumor extended beyond the bone and into an adjacent chamber?
When
sampling the tumor, submit sections to demonstrate the relationship of the
tumor to the surrounding mucosa and the underlying bone. In addition, submit
sections to determine tumor spread into adjacent anatomic structures and
com-partments. For example, the nasal mucosa should be amply sampled for tumors
involving the medial maxillary wall. If an eye is included in a resection of
the superior wall of the maxilla,
submit
sections of the orbital contents. For the eye itself, one section (in addition
to the optic nerve margin) is generally sufficient to document its presence and
to demonstrate its relationship to the tumor.
Regional
lymph nodes are usually removed separately by the surgeon and submitted as
sepa-rate specimens. They should be anatomically oriented, and each level
should be carefully dis-sected . Each lymph node should be submitted for
histologic evaluation.
Important Issues to Address in Your Surgical Pathology Report on Maxillary Sinus Resections
What
procedure was performed, and what structures/organs are present?
· Is a
neoplasm present?
· What is
the probable site of tumor origin (max-illary sinus, maxillary bone, palate,
nasal cavity)? For tumors of the maxillary sinus, from what surface does the
tumor arise (inferior, superior, medial, lateral, anterior, posterior)?
· What is
the size of the tumor (in centimeters), and what is the greatest depth of tumor
inva-sion?
· What are
the histologic type and grade of the tumor? Is an in situ component present?
· Does the
tumor extend into bone? If so, does the tumor extend beyond the bony confines
of the maxillary sinus to involve adjacent compartments and structures (e.g.,
nasal cavity, oral cavity, orbital cavity, skin, ptery-goid complex)?
· Does the
tumor involve the margins (mucosal, skin, bone, soft tissues)?
·
Does the tumor involve regional lymph nodes?
Include the number of nodes examined and the number of nodes involved.
Related Topics