Chapter: Pathology: Hematopoetic Pathology–White Blood Cell Disorders & Lymphoid and Myeloid Neoplasms
Mature B-Cell Neoplasms
MATURE B-CELL NEOPLASMS
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are very similar; they both represent an abnormal
proliferation of B cells. Patients who pres-ent with lymph node findings are classified as having SLL. Patients who
present with blood findings are
classified as having CLL; 50% of CLL patients also have lymph node involvement.
•
CLL is the most indolent of all of the leukemias.
•
Mean age at time of diagnosis is age 60.
•
The malignant cells are nonfunctional, so patients develop
hypogammaglobu-linemia, leading to an increased risk of infections.
•
CLL is associated with warm autoimmune hemolytic anemia (AIHA) (10% of
cases), which will cause spherocytes to be observed in peripheral blood.
•
CLL rarely transforms into a worse disease such as prolymphocytic
leukemia or large cell lymphoma (Richter syndrome).
CLL and SLL can be categorized
by the markers present on the B cells:
•
B-chronic lymphocytic leukemia cells (95% of cases) have B-cell markers,
such as CD19 and CD20. One T-cell marker, CD5, is also present. Also important
is that the cells are CD23 positive and CD10 negative.
•
SLL occurs only as this type.
•
T-chronic lymphocytic leukemia cells (5% of cases) have T-cell markers.
The histology of affected lymph nodes reveals only a diffuse pattern (not
nodular), but proliferation centers may also be present.
•
Peripheral blood findings show increased numbers of normal-appearing
lym-phocytes. Numerous smudge cells (“parachute cells”) are also present; the
smudge cells result from the fact that the neoplastic lymphocytes are
unusu-ally fragile.
•
Bone marrow shows numerous normal-appearing neoplastic lymphocytes.
Hairy cell leukemia is a rare
B-cell neoplasm that causes indolent disease in middle-aged Caucasian men.
There can be a “dry tap” with bone marrow aspiration. Lym-phocytes have
“hairlike” cytoplasmic projections; the diagnostic stain is positive
tartrate-resistant acid phosphatase (TRAP).
Physical examination shows a
markedly enlarged spleen (splenomegaly) due to infil-tration of red pulp by
malignant cells.
Treatment is
2-chloro-deoxyadenosine (2-CdA), which inhibits adenosine deami-nase (ADA) and
increases levels of toxic deoxyadenosine.
Follicular lymphoma is a
well-differentiated B -cell lymphoma with follicular archi-tecture. All
follicular lymphomas are derived from B lymphocytes.
•
Most common form of non-Hodgkin lymphoma in the United States
•
Characteristic translocation is t(14;18), involving the immunoglobulin
heavy chain gene and BCL2 gene (activation of bcl-2 inhibits apoptosis by
blocking the bax channel)
•
Frequently presents with disseminated disease (more advanced stage)
•
Prognosis is better than diffuse lymphoma, but it doesn’t respond to
therapy (unlike the more aggressive diffuse non-Hodgkin lymphomas)
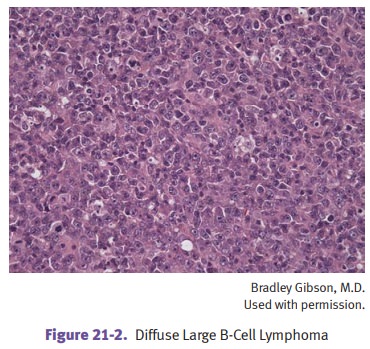
Diffuse large B-cell lymphoma is
a high grade large B-cell lymphoma with a diffuse growth pattern. It is an
aggressive, rapidly proliferating tumor which may respond to therapy. Special
subtypes include immunodeficiency-associated B-cell lymphomas (often infected
with Epstein-Barr virus) and body-cavity large B-cell lymphomas (sometimes
associated with human herpes virus [HHV]-8).
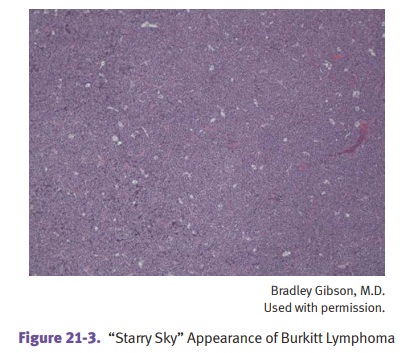
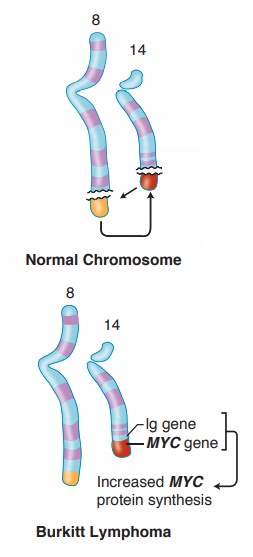
Small noncleaved lymphoma (Burkitt lymphoma) is a high
grade B-cell lymphoma. It is composed of
intermediate-sized lymphoid cells with a “starry sky” appearance due to
numerous reactive tingible-body macrophages (phagocytosis of apoptotic tumor
cells). There is a characteristic t(8;14) translocation juxtaposing MYC to the
immunoglobulin heavy chain locus in most cases.
•
African
type: endemic form
°°
Involvement of mandible or maxilla is characteristic; is associated
with Epstein-Barr virus
•
American
type: nonendemic, sporadic form
°°
Involvement of the abdomen (such as bowel, retroperitoneum, or
ova-ries); has a high incidence in AIDS patients
Both endemic and sporadic
forms of Burkitt lymphoma are seen most often in children and young adults.
Mantle cell lymphoma (MCL) is a rare B-cell lymphoma in
which the tumor cells arise from mantle zone B
lymphocytes (positive for CD19, CD20, and CD5; nega-tive for CD23). The
characteristic translocation is t(11;14), involving CCD1 and the heavy chain locus.
Marginal zone lymphoma (MALToma) is a diverse group of B-cell
neoplasms that arise within lymph nodes,
spleen, or extranodal tissue. It is associated with mucosa-associated lymphoid
tissue (MALTomas). The lesion begins as a reactive polyclonal reaction and may
be associated with previous autoimmune disorders or infectious disease (e.g.,
Sjögren disease, Hashimoto thyroiditis, Helicobacter
gastritis). The lymphoma remains localized for long periods of time.
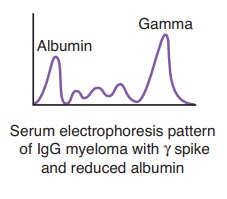
Multiple myeloma is a malignant neoplasm of plasma cells.
•
Most common primary tumor arising in the bone marrow of adults
•
Lab studies show increased serum protein with normal serum albumin;
an M spike in serum electrophoresis is a monoclonal immunoglobulin spike—most
commonly IgG (60%) and next most commonly IgA (20%)
•
Bence Jones proteins are light chains that are small and can be
filtered into urine.
Histologically, bone marrow
shows increased plasma cells (>20% is characteristic). Peripheral blood may
show rouleaux formation (“stack of coins”). Multiple lytic bone lesions are due
to the osteoclastic activating factor. Lytic bone lesions cause hypercalcemia,
bone pain, and increased risk of fracture.
Increased risk of infection
is the most common cause of death. Other complications include renal disease
(such as myeloma nephrosis) and primary amyloidosis (10% of patients) due to
amyloid light (AL) chains. Increased amounts of IL-6 are associated with a
poorer prognosis because survival of myeloma cells is dependent on IL-6.
Plasmacytoma is a solitary myeloma within bone or soft
tissue.
•
Within bone: precursor lesion that can later
develop into myeloma
•
Outside bone (extramedullary): usually
found within upper respiratory tract
Monoclonal gammopathy of undetermined significance (MGUS) (an old name was benign monoclonal gammopathy).
Serum M protein is found in 1–3% of asymp-tomatic individuals age >50; the
incidence increases with increasing age. The annual risk of developing a plasma
cell dyscrasia, usually multiple myeloma, is 1–2% per year. MGUS may also
evolve into Waldenström macroglobulinemia, primary amy-loidosis, B-cell lymphoma,
or CLL.
Lymphoplasmacytic lymphoma (Waldenström macroglobulinemia) is a small
lym-phocytic lymphoma with plasmacytic differentiation. It is a cross between
multiple myeloma and SLL.
Like myeloma, it has an M
spike (IgM). Like SLL (and unlike myeloma), the neo-plastic cells infiltrate
many organs (e.g., lymph nodes, spleen, bone marrow). Also unlike multiple
myeloma, there are no lytic bone lesions and there is no increase in serum
calcium. Russell bodies (cytoplasmic immunoglobulin) and Dutcher bodies
(intranuclear immunoglobulin) may be present.
•
May have hyperviscosity syndrome, because IgM is a large pentamer
•
Visual abnormalities may be due to vascular dilatations and hemorrhages
in the retina
•
Neurologic symptoms include headaches and confusion
•
Bleeding and cryoglobulinemia can be due to abnormal globulins, which
pre-cipitate at low temperature and may cause Raynaud phenomenon
Related Topics