Chapter: Clinical Cases in Anesthesia : Aortic Stenosis
How is hypotension best treated in the patient with aortic stenosis?
How is
hypotension best treated in the patient with aortic stenosis?
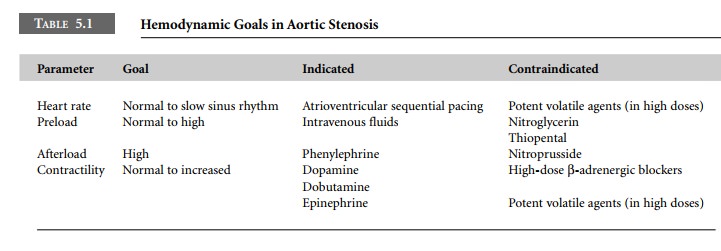
Patients with severe AS do not tolerate
hypotension, and even brief episodes may lead to hemodynamic decompen-sation.
The determinants of cardiac output are preload, afterload, heart rate, and
contractility (Table 5.1). The pri-orities of treatment should be the
following:
·
preservation
of blood pressure using vasoconstrictors to increase afterload
·
restoration
of sinus rhythm and intravenous fluids to maintain preload
·
maintaining
a heart rate in the normal range
·
maintenance
of myocardial contractility
Treatment of Supraventricular Dysrhythmias
Tachydysrhythmias
Therapeutic diagnostic maneuvers
Vagal
maneuvers
Adenosine
Treatment
β-Adrenergic
blockers
Amiodarone
Cardioversion
Bradydysrhythmias
Anticholinergics
α- and β-adrenergic
agonists
Atrioventricular
sequential pacing
If the etiology is not immediately obvious,
then empiric treatment with an α-adrenergic receptor agonist (phenyle-phrine)
should be attempted. The goal is to preserve CPP so that the heart does not
enter a vicious cycle of irre-versible ischemia. In general, pure α-adrenergic receptor agonists are the preferred vasoconstrictor
agents because they do not cause tachycardia. In this way, the CPP is increased
and diastolic filling time is maintained
Related Topics