Chapter: Psychiatric Mental Health Nursing : Client’s Response to Illness
Cultural Factors - Client’s Response to Illness
CULTURAL FACTORS
According to the U.S. Census Bureau, 33% of U.S. resi-dents
currently are members of nonwhite cultures. By 2050, the nonwhite population
will more than triple. This changing composition of society has implications
for health-care professionals, who are predominantly white and unfamiliar with
different cultural beliefs and practices (Purnell & Paulanka, 2008). Culturally competent nurs-ing care
means being sensitive to issues related to culture, race, gender, sexual
orientation, social class, economic situ-ation, and other factors.
Nurses and other health-care providers must learn about other
cultures and become skilled at providing care to people with cultural
backgrounds that are different from their own. Finding out about another’s
cultural beliefs and practices and understanding their meaning is essential to
providing holistic and meaningful care to the client (Table 7.3).
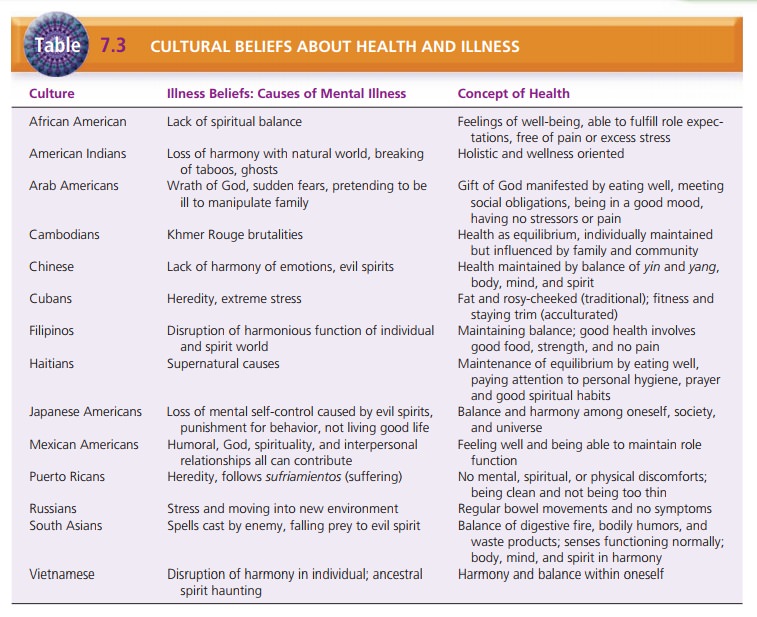
Beliefs About Causes of Illness
Culture has the most influence on a person’s health beliefs and
practices. It has been shown to influence one’s concept of disease and illness.
Two prevalent types of beliefs about what causes illness in non-Western
cultures are natural and unnatural or personal. Unnatural or personal
beliefs attribute the cause of illness to the active, purposeful intervention
of an outside agent, spirit, or supernatural force or deity. The natural view is rooted in a belief that
natural conditions or forces, such as
cold, heat, wind, or dampness, are responsible for the illness (Giger &
Davidhizar, 2007). A sick person with these beliefs would not see the
relationship between his or her behavior or health practices and the illness.
Thus, he or she would try to counteract the negative forces or spirits using
traditional cultural remedies rather than taking medi-cation or changing his or
her health practices.
Factors in Cultural Assessment
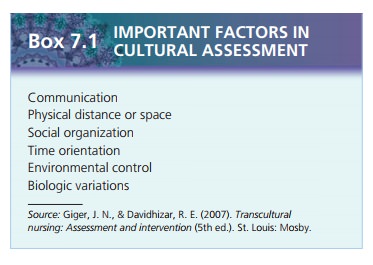
Giger and Davidhizar (2007) recommended a model for assessing
clients using six cultural phenomena: communication, physical distance or
space, social or-ganization, time orientation, environmental control, and
biologic variations. Each phenomenon is discussed in more detail below and in
Table 7.4.
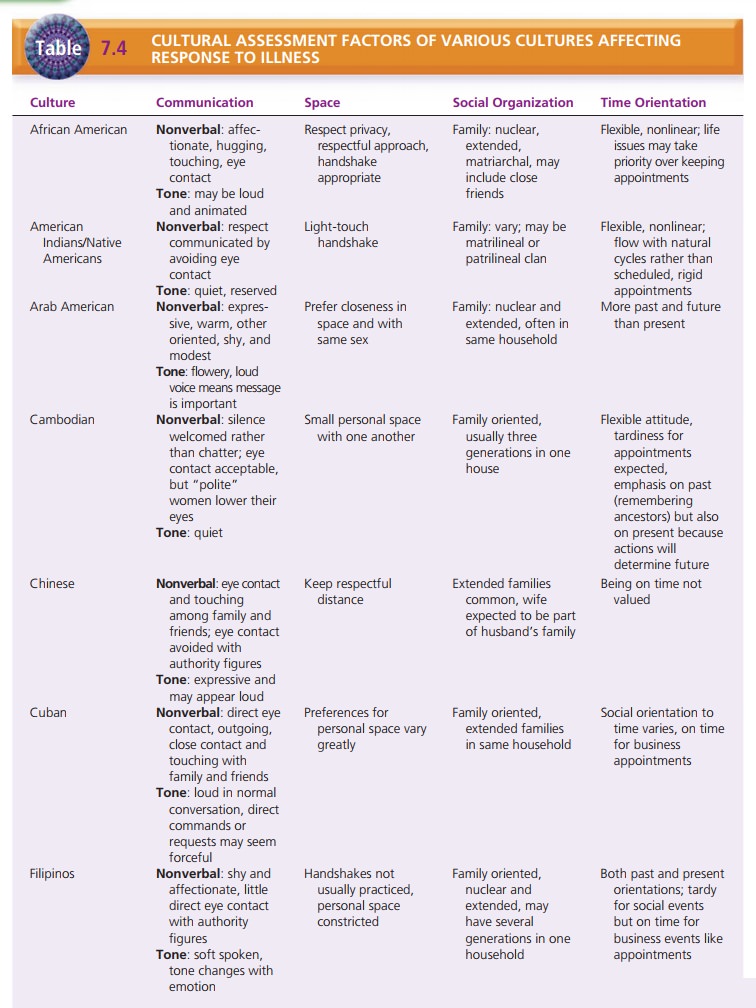
Communication
Verbal communication can be difficult when the client and nurse do
not speak the same language. The nurse should be aware that nonverbal
communication has different meanings in various cultures. For example, some
cultures welcome touch and consider it supportive, whereas other cultures find
touch offensive. Some Asian women avoid shaking hands with one another or men.
Some Native American tribes believe that vigorous handshaking is aggressive,
whereas peo-ple from Spain and France consider a firm handshake a sign of
strength and good character.
Although Western cultures view direct eye contact as positive,
Native American and Asian cultures may find it rude, and people from these
backgrounds may avoid look-ing strangers in the eye when talking to them.
People from Middle Eastern cultures can maintain very intense eye contact,
which may appear to be glaring to those from dif-ferent cultures.
Physical Distance or Space
Various cultures have different perspectives on what they consider
a comfortable physical distance from another person during communication. In
the United States and many other Western cultures, 2 to 3 feet is a comfortable
distance. Latin Americans and people from the Middle East tend to stand closer
to one another than do people in Western cultures. People from Asian and Native
Ameri-can cultures are usually more comfortable with distances greater than 2
or 3 feet. The nurse should be conscious of these cultural differences in space
and should allow enough room for clients to be comfortable (Giger &
Davidhizar, 2007).
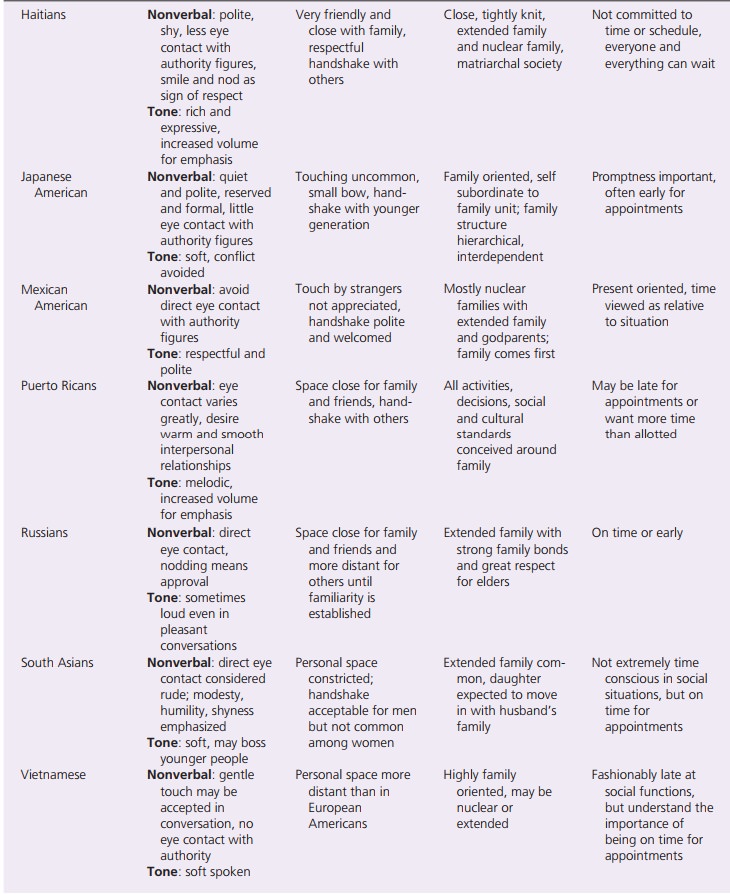
Social Organization
Social organization refers to family structure
and organi-zation, religious values and beliefs, ethnicity, and culture, all of
which affect a person’s role and, therefore, his or her health and illness
behavior. In Western cultures, people may seek the advice of a friend or family
member or may make most decisions independently. Many Chinese, Mexi-can,
Vietnamese, and Puerto Rican Americans strongly value the role of family in making
health-care decisions. People from these backgrounds may delay making
deci-sions until they can consult appropriate family members. Autonomy in
health-care decisions is an unfamiliar and undesirable concept because the
cultures consider the col-lective to be greater than the individual.
Time Orientation
Time orientation, or whether one views time
as precise or approximate, differs
among cultures. Many Westerncountries focus on the urgency of time, valuing
punctuality and precise schedules. Clients from other cultures may not perceive
the importance of adhering to specific follow-up appointments or procedures or
time-related treatment regi-mens. Health-care providers can become resentful
and angry when these clients miss appointments or fail to fol-low specific
treatment regimens such as taking medications at prescribed times. Nurses
should not label such clients as noncompliant when their behavior may be
related to a dif-ferent cultural orientation to the meaning of time. When
possible, the nurse should be sensitive to the client’s time orientation, as
with follow-up appointments. When timing is essential, as with some
medications, the nurse can explain the importance of more precise timing.
![]()
![]()
Environmental Control
Environmental control refers to a client’s ability
to control the surroundings or
direct factors in the environment (Giger & Davidhizar, 2007). People who
believe they have control of their health are more likely to seek care, to
change their behavior, and to follow treatment recommen-dations. Those who
believe that illness is a result of nature or natural causes are less likely to
seek traditional health care because they do not believe it can help them.
Biologic Variations
Biologic variations exist among people from different cul-tural backgrounds,
and research is just beginning to help us understand these variations. For
example, we now know that differences related to ethnicity/cultural origins cause variations in response to some
psychotropic drugs (discussed earlier). Biologic variations based on physical
makeup are said to arise from one’s race,
whereas other cultural variations arise from ethnicity. For example, sickle
cell anemia is found almost exclusively in African Ameri-cans, and Tay-Sachs
disease is most prevalent in the Jewish community.
Socioeconomic Status and Social Class
Socioeconomic status refers to one’s income,
education, and occupation. It
strongly influences a person’s health, including whether or not the person has
insurance and adequate access to health care or can afford prescribed
treatment. People who live in poverty are also at risk for threats to health,
such as inadequate housing, lead paint, gang-related violence, drug
trafficking, or substandard schools.
Social class has less influence in the United States, where
barriers among the social classes are loose and mobility is common: people can
gain access to better schools, housing, health care, and lifestyle as they
increase their income. In many other countries, however, social class is a
powerful influence on social relationships and can determine how people relate
to one another, even in a health-care setting. For example, the caste system
still![]()
![]() exists in India, and people in the lowest caste
may feel unworthy or undeserving of the same level of health care as people in
higher castes. The nurse must determine whether social class is a factor in how
clients relate to health-care providers and the health-care system.
exists in India, and people in the lowest caste
may feel unworthy or undeserving of the same level of health care as people in
higher castes. The nurse must determine whether social class is a factor in how
clients relate to health-care providers and the health-care system.
Related Topics