Chapter: Medical Surgical Nursing: Management of Patients With Upper Respiratory Tract Disorders
Epistaxis (Nosebleed) - Upper Respiratory Airway
EPISTAXIS (NOSEBLEED)
A
hemorrhage from the nose, referred to as epistaxis,
is caused by the rupture of tiny, distended vessels in the mucous membrane of
any area of the nose. Rarely does epistaxis originate in the densely vascular
tissue over the turbinates. Most commonly, the site is the anterior septum,
where three major blood vessels enter the nasal cavity: (1) the anterior
ethmoidal artery on the forward part of the roof (Kesselbach’s plexus), (2) the
sphenopalatine artery in the posterosuperior region, and (3) the internal
maxil-lary branches (the plexus of veins located at the back of the lateral
wall under the inferior turbinate).
There
are a variety of causes associated with epistaxis, including trauma, infection,
inhalation of illicit drugs, cardiovascular dis-eases, blood dyscrasias, nasal
tumors, low humidity, a foreign body in the nose, and a deviated nasal septum.
Additionally, vigorous nose blowing and nose picking have been associated with
epistaxis.
Medical Management
Management of epistaxis depends on the location of the bleeding site. A nasal speculum or headlight may be used to determine the site of bleeding in the nasal cavity. Most nosebleeds originate from the anterior portion of the nose. Initial treatment may in-clude applying direct pressure. The patient sits upright with the head tilted forward to prevent swallowing and aspiration of blood and is directed to pinch the soft outer portion of the nose against the midline septum for 5 or 10 minutes continuously. If this mea-sure is unsuccessful, additional treatment is indicated. In anterior nosebleeds, the area may be treated with a silver nitrate applica-tor and Gelfoam, or by electrocautery. Topical vasoconstrictors, such as adrenaline (1 1,000), cocaine (0.5%), and phenylephrine may be prescribed.
If
bleeding is occurring from the posterior regions, cotton pledgets soaked in a
vasoconstricting solution may be inserted into the nose to reduce the blood
flow and improve the exam-iner’s view of the bleeding site. Alternatively, a
cotton tampon may be used to try to stop the bleeding. Suction may be used to
remove excess blood and clots from the field of inspection. The search for the
bleeding site should shift from the anteroinferior quadrant to the
anterosuperior, then to the posterosuperior, and finally to the posteroinferior
area. The field is kept clear by using suction and by shifting the cotton
tampon. Only about 60% of the total nasal cavity can actually be seen, however.
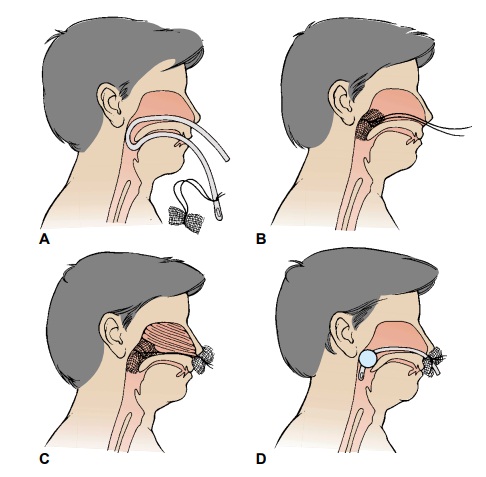
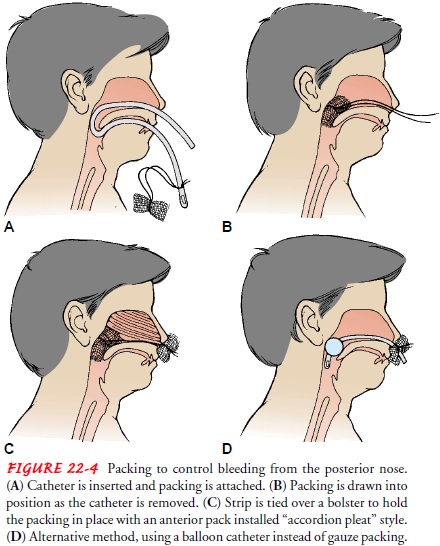
When
the origin of the bleeding cannot be identified, the nose may be packed with
gauze impregnated with petrolatum jelly or antibiotic ointment; a topical
anesthetic spray and decongestant agent may be used prior to inserting the
gauze packing, or a balloon-inflated catheter may be used (Fig. 22-4). The
packing may remain in place for 48 hours or up to 5 or 6 days if necessary to
control bleeding. Antibiotics may be prescribed because of the risk of
iatrogenic sinusitis and toxic shock syndrome.
Nursing Management
The
nurse monitors the vital signs, assists in the control of bleed-ing, and
provides tissues and an emesis basin to allow the patient to expectorate any
excess blood. It is not uncommon for patients to be anxious in response to a
nosebleed. Blood loss on clothing and handkerchiefs can be frightening, and the
nasal examination and treatment are uncomfortable. Assuring the patient in a
calm, efficient manner that bleeding can be controlled can help reduce anxiety.
TEACHING PATIENTS SELF-CARE
Discharge teaching includes reviewing ways to prevent epistaxis: avoiding forceful nose blowing, straining, high altitudes, and nasal trauma (including nose picking).
Adequate humidification may prevent drying of
the nasal passages. The nurse instructs the patient how to apply direct
pressure to the nose with the thumb and the index finger for 15 minutes in the
case of a recurrent nosebleed. If recurrent bleeding cannot be stopped, the
patient is instructed to seek additional medical attention.
Related Topics