Chapter: Psychiatric Mental Health Nursing : Neurobiologic Theories and Psychopharmacology
Antianxiety Drugs (Anxiolytics) - Psychopharmacology
Antianxiety Drugs (Anxiolytics)
Antianxiety drugs, or anxiolytic drugs, are used to treat anxiety and anxiety disorders, insomnia, OCD, depression, posttraumatic stress disorder, and alcohol withdrawal. Antianxiety drugs are among the most widely prescribed medications today. A wide variety of drugs from different classifications have been used in the treatment of anxiety and insomnia. Benzodiazepines have proved to be the most effective in relieving anxiety and are the drugs most frequently prescribed. Benzodiazepines also may be prescribed for their anticonvulsant and muscle relaxant effects. Buspirone is a nonbenzodiazepine often used for the relief of anxiety and therefore is included in this section. Other drugs such as propranolol, clonidine (Catapres), and hydroxyzine (Vistaril) that may be used to relieve anxiety are much less effective and are not included in this discussion.
![]()
![]()
Mechanism of Action
Benzodiazepines mediate the actions of the amino acid GABA, the
major inhibitory neurotransmitter in the brain. Because GABA receptor channels
selectively admit the anion chloride into neurons, activation of GABA receptors
hyperpolarizes neurons and thus is inhibitory. Benzodiaz-epines produce their
effects by binding to a specific site on the GABA receptor. Buspirone is
believed to exert its anxi-olytic effect by acting as a partial agonist at
serotonin receptors, which decreases serotonin turnover (Arniel & Mathew,
2007).
The benzodiazepines vary in terms of their half-lives, the means by
which they are metabolized, and their effec-tiveness in treating anxiety and
insomnia. Table 2.6 lists dosages, half-lives, and speed of onset after a
single dose. Drugs with a longer half-life require less frequent dosing and
produce fewer rebound effects between doses; how-ever, they can accumulate in
the body and produce “next-day sedation” effects. Conversely, drugs with a
shorter half-life do not accumulate in the body or cause next-day sedation, but
they do have rebound effects and require more frequent dosing.
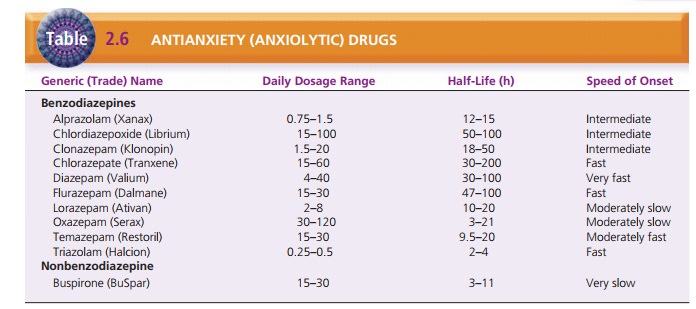
Temazepam (Restoril), triazolam (Halcion), and flu-razepam
(Dalmane) are most often prescribed for sleep rather than for relief of
anxiety. Diazepam (Valium), chlordiazepoxide (Librium), and clonazepam often are
used to manage alcohol withdrawal as well as to relieve anxiety.
Side Effects
Although not a side effect in the true sense, one chief prob-lem
encountered with the use of benzodiazepines is their tendency to cause physical
dependence. Significant dis-continuation symptoms occur when the drug is
stopped; these symptoms often resemble the original symptoms for which the
client sought treatment. This is especially a problem for clients with
long-term benzodiazepine use, such as those with panic disorder or generalized
anxiety disorder. Psychological dependence on benzodiazepines is common:
Clients fear the return of anxiety symptoms or believe they are incapable of
handling anxiety without the drugs. This can lead to overuse or abuse of these
drugs. Buspirone does not cause this type of physical dependence.
The side effects most commonly reported with benzodi-azepines are
those associated with CNS depression, such as drowsiness, sedation, poor
coordination, and impaired memory or clouded sensorium. When used for sleep,
cli-ents may complain of next-day sedation or a hangover effect. Clients often
develop a tolerance to these symp-toms, and they generally decrease in
intensity. Common side effects from buspirone include dizziness, sedation,
nausea, and headache (Arniel & Mathew, 2007).
Elderly clients may have more difficulty managing the effects of
CNS depression. They may be more prone to falls from the effects on
coordination and sedation. They also may have more pronounced memory deficits
and may have problems with urinary incontinence, particularly at night.
Client Teaching
Clients need to know that antianxiety agents are aimed at relieving
symptoms such as anxiety or insomnia but do not treat the underlying problems
that cause the anxiety. Ben-zodiazepines strongly potentiate the effects of
alcohol: One drink may have the effect of three drinks. Therefore, clients
should not drink alcohol while taking benzodiazepines. Clients should be aware
of decreased response time, slower reflexes, and possible sedative effects of
these drugs when attempting activities such as driving or going to work.
Benzodiazepine withdrawal can be fatal. After the client has
started a course of therapy, he or she should never discontinue benzodiazepines
abruptly or without the supervision of the physician (Lehne, 2006).
Related Topics