Chapter: Medical Surgical Nursing: Assessment of Renal and Urinary Tract Function
X-Ray Films and Other Imaging Modalities - Renal and Urinary Tract Function
X-RAY
FILMS AND OTHER IMAGING MODALITIES
Kidney, Ureter, and Bladder Studies
An
x-ray study of the abdomen or kidney, ureters, and bladder (KUB) may be
performed to delineate the size, shape, and posi-tion of the kidneys and to
reveal any abnormalities, such as calculi (stones) in the kidneys or urinary
tract, hydronephrosis (distention of the pelvis of the kidney), cysts, tumors,
or kidney displacement by abnormalities in surrounding tissues.
General Ultrasonography
Ultrasonography is a noninvasive procedure that uses sound waves passed into the body through a transducer to detect abnormalities of internal tissues and organs. Structures of the urinary system cre-ate characteristic ultrasonographic images. Abnormalities such as fluid accumulation, masses, congenital malformations, changes in organ size, or obstructions can be identified. During the test, the lower abdomen and genitalia may need to be exposed. Ultra-sonography requires a full bladder; therefore, fluid intake should be encouraged before the procedure. Because of its sensitivity, ultra sonography has replaced many other tests as the initial diagnostic procedure.
Bladder Ultrasonography
Bladder ultrasonography is a noninvasive method of measuring urine volume in the bladder. It may be indicated for urinary fre-quency, inability to void after removal of an indwelling urinary catheter, measurement of postvoiding residual urine volume, in-ability to void postoperatively, or assessment of the need for catheterization during the initial stages of an intermittent catheter-ization training program. Portable, battery-operated devices are available for bedside use. The scan head is placed on the patient’s abdomen and directed toward the bladder. The device automat-ically calculates and displays urine volume.
Computed Tomography and Magnetic Resonance Imaging
Computed
tomography (CT) and magnetic resonance imaging (MRI) are noninvasive techniques
that provide excellent cross-sectional views of the kidney and urinary tract.
They are used in evaluating genitourinary masses, nephrolithiasis, chronic
renal infections, renal or urinary tract trauma, metastatic disease, and soft
tissue abnormalities. The nurse should explain to the patient that a sedative
may be prescribed. Claustrophobia is often a problem, especially with MRI.
Patient preparation for the MRI includes removal of any metallic objects, such
as jewelry or cloth-ing with metallic clasps. Credit cards should be kept away
from the MRI area because of their magnetic strips. MRI is con-traindicated in
patients with pacemakers, surgical clips, or any metallic objects anywhere in
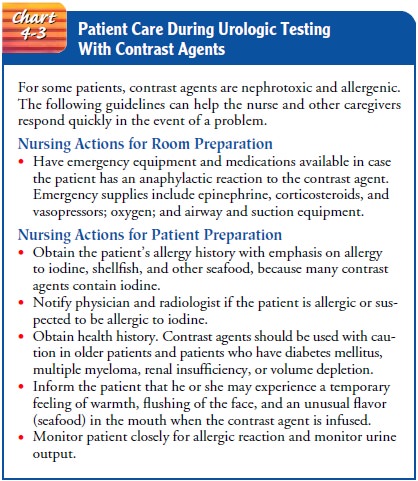
the body. Occasionally, an oral or intravenous radiopaque contrast material is
used in CT scanning to enhance visualization. Nursing care guidelines for
patient preparation and test precautions for any imaging procedure re-quiring a
contrast agent (also called contrast medium) are ex-plained in Chart 43-3.
Nuclear Scans
Nuclear
scans require injection of a radioisotope (technetium-99m–labeled compound or
iodine-131 hippurate) into the cir-culatory system; the isotope is then monitored
as it moves through the blood vessels of the kidneys. A scintillation camera is
placed behind the kidney with the patient in a supine, prone, or seated
position. Hypersensitivity to the radioisotope is rare. The technetium scan
provides information about kidney perfusion; the hippurate scan provides
information about kidney function.
Nuclear
scans are used to evaluate acute and chronic renal fail-ure, renal masses, and
blood flow before and after kidney trans-plantation. The radioisotope is
injected at a specified time before the study to achieve the proper
concentration in the kidneys. After the procedure is completed, the patient is
encouraged to drink flu-ids to promote excretion of the radioisotope by the
kidneys.
Intravenous Urography
Intravenous
urography includes various tests such as excretory urog-raphy, intravenous
pyelography (IVP), and infusion drip pyelogra-phy. A radiopaque contrast agent
is administered intravenously. An IVP, or intravenous urogram, shows the
kidneys, ureter, and blad-der via x-ray imaging as dye moves through the upper
and then lower urinary system. A nephrotomogram may be carried out as part of
the study to visualize different layers of the kidney and the diffuse structures
within each layer and to differentiate solid masses or lesions from cysts in
the kidneys or urinary tract.
Intravenous
urography may be used as the initial assessment of any suspected urologic
problem, especially lesions in the kid-neys and ureters. It also provides a
rough estimate of renal func-tion. After the contrast agent (sodium diatrizoate
or meglumine diatrizoate) is administered intravenously, multiple x-rays are
ob-tained to visualize drainage structures.
Infusion
drip pyelography requires an intravenous infusion of a large volume of a dilute
contrast agent to opacify the renal parenchyma and fill the urinary tract. This
examination method is useful when prolonged opacification of the drainage
structures is desired so that tomograms (body-section radiography) can be made.
Images are obtained at specified intervals after the start of the infusion.
These images show the filled and distended collect-ing system. The patient
preparation is the same as for excretory urography, except that fluids are not
restricted.
Retrograde Pyelography
In retrograde
pyelography, catheters are advanced through the ureters into the renal pelvis
by means of cystoscopy. A contrast agent is then injected. Retrograde
pyelography is usually per-formed if intravenous urography provides inadequate
visual-ization of the collecting systems. It may also be used before
extracorporeal shock-wave lithotripsy or in patients with urologic cancer who
need follow-up and are allergic to intravenous contrast agents. Possible
complications include infection, hematuria, and perforation of the ureter.
Retrograde pyelography is used infre-quently because of improved techniques in
excretory urography.
Cystography
Cystography
aids in evaluating vesicoureteral reflux (backflow of urine from the bladder
into one or both ureters) and assessing the patient for bladder injury. A
catheter is inserted into the bladder, and a contrast agent is instilled to
outline the bladder wall. The con-trast agent may leak through a small bladder
perforation stem-ming from bladder injury, but such leakage is usually
harmless. Cystography can also be performed with simultaneous pressure
recordings inside the bladder.
Voiding Cystourethrography
Voiding
cystourethrography uses fluoroscopy to visualize the lower urinary tract and
assess urine storage in the bladder. It is commonly used as a diagnostic tool
to identify vesicoureteral reflux (between bladder and ureter). A urethral
catheter is inserted, and a contrast agent is instilled into the bladder. When
the bladder is full and the patient feels the urge to void, the catheter is
removed, and the pa-tient voids. Retrograde urethrography, in which a contrast
agent is injected retrograde into the urethra, is always performed before
ure-thral catheterization if urethral trauma is suspected.
Renal Angiography
A
renal angiogram, or renal arteriogram, provides an image of the renal arteries.
The femoral (or axillary) artery is pierced with a needle, and a catheter is
threaded up through the femoral and iliac arteries into the aorta or renal
artery. A contrast agent is in-jected to opacify the renal arterial supply.
Angiography is used toevaluate renal blood flow in suspected renal trauma, to
differen-tiate renal cysts from tumors, and to evaluate hypertension. It is
used preoperatively for renal transplantation. Before the proce-dure, a
laxative may be prescribed to evacuate the colon so that unobstructed x-rays
can be obtained. Injection sites (groin for femoral approach or axilla for
axillary approach) may be shaved. The peripheral pulse sites (radial, femoral, and
dorsalis pedis) are marked for easy access during postprocedural assessment.
The pa-tient is informed that there may be a brief sensation of heat along the
course of the vessel when the contrast agent is injected.
After
the procedure, vital signs are monitored until stable. If the axillary artery
was the injection site, blood pressure measurements are taken on the opposite
arm. The injection site is examined for swelling and hematoma. Peripheral
pulses are palpated, and the color and temperature of the involved extremity
are noted and com-pared with those of the uninvolved extremity. Cold compresses
may be applied to the injection site to decrease edema and pain. Possible
complications include hematoma formation, arterial thrombosis or dissection,
false aneurysm formation, and altered renal function.
Related Topics