Chapter: Pathology: Female Genital Pathology
Uterus - Pathology
UTERUS
Endometritis is inflammation of the endometrial
lining in the uterus. It can be acute or chronic.
•
Acute
endometritis is
an ascending infection from the cervix; it is associated with pregnancy and abortion.
•
Chronic
endometritis is
associated with PID and intrauterine devices; plasma
cells
are seen in the endometrium.
Endometriosis is the presence of endometrial
glands and stroma outside the uterus.
It
most commonly affects women of reproductive age. Common sites of involvement
are the ovaries, ovarian and uterine ligaments, pouch of Douglas, serosa of
bowel and urinary bladder, and peritoneal cavity. It can present with chronic
pelvic pain, dysmenorrhea and dyspareunia, rectal pain and constipation,
abnormal uterine bleeding, or infertility.
Grossly,
endometriosis causes red-brown serosal nodules (an endometrioma is an ovarian “chocolate” (hemolyzed blood) cyst).
Leiomyoma (fibroid), the most
common tumor of the female genital tract, is a benign, smooth muscle tumor of
the myometrium. Leiomyomas have a high incidence in African Americans, though
they are common across all populations. Their growth is estrogen-dependent.
Leiomyomas may present with
menorrhagia, abdominal mass, pelvic/back pain, suprapubic discomfort, or
infertility and spontaneous abortion.
Grossly, leiomyomas form
well-circumscribed, rubbery, white-tan masses with a whorled, trabeculated
appearance on cut section. Leiomyomas are commonly mul-tiple, and may have
subserosal, intramural, and submucosal location. The malignant variant is
leiomyosarcoma.
Endometrial hyperplasia refers
to a histological proliferation of endometrial glands with 2 important
histopathologic categories:
•
Benign endometrial hyperplasia shows uniform remodeling of glands with
cyst formation.
•
Endometrial intraepithelial neoplasia shows crowded architecture and
cyto-logic alteration on biopsy.
o
Patients are at high risk for endometrial adenocarcinoma.
o
Treatment options include total hysterectomy or progestin therapy with
biopsy surveillance.
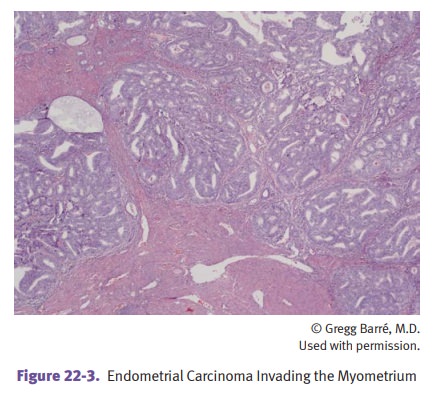
Endometrial adenocarcinoma is
the most common malignant tumor of the lower female genital tract. It most
commonly affects postmenopausal women who present with abnormal uterine
bleeding. Risk factors are mostly related to estrogen:
•
Early menarche and late menopause
•
Nulliparity
•
Hypertension and diabetes
•
Obesity
•
Chronic anovulation
•
Estrogen-producing ovarian tumors (granulosa cell tumors)
•
ERT and tamoxifen
•
Endometrial hyperplasia (complex atypical hyperplasia)
•
Lynch syndrome (colorectal, endometrial, and ovarian cancers)
Endometrial adenocarcinoma
typically forms a tan polypoid endometrial mass; invasion of myometrium is
prognostically important.
•
Endometroid adenocarcinoma (most common histological type): associated
with PTEN mutations
•
Serous tumors: associated with TP53 mutations
Less common types of uterine malignancy include leiomyosarcoma, a malignant, smooth muscle tumor, and carcinosarcoma, which contains both malignant
stromal cells and endometrial adenocarcinoma.
Adenomyosis is an invagination of the deeper
layers of the endometrium into the myometrium, which
causes menorrhagia and dysmenorrhea.
Anovulation can
cause abnormal uterine bleeding, especially in women near men-arche and
menopause. Biopsy shows glandular and stromal breakdown in a back-ground of
proliferative phase endometrium.
Related Topics