Chapter: Medicine and surgery: Genitourinary system
Urinary tract obstruction - Renal tract obstruction
Renal tract obstruction
Urinary tract obstruction
Definition
Obstruction of the urinary tract at any level, whether partial or complete, can cause symptoms and renal impairment.
Aetiology
The likely causes depend on the age of the patient and the level of obstruction. In children, abnormal anatomy such as urethral valves or stenosis is most likely, whereas stones are more likely in adults. In older men prostatic
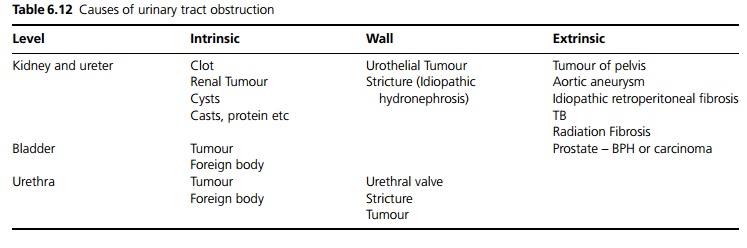
hypertrophy or carcinoma are most common. With increasing age in both sexes retroperitoneal or pelvic malignancy should be suspected. See Table 6.12.
Pathophysiology
If urine continues to be produced, obstruction causes a rise in pressure and dilatation of the proximal part of the urinary tract. The effects of obstruction depend on the site, severity and rate of onset of obstruction.
┬Ę Renal obstruction usually causes loin pain, whereas bladder outflow obstruction may cause a sensation of a full bladder.
┬Ę If both kidneys are completely obstructed (either at the level of the ureters (uncommon) or because of bladder outflow obstruction), or if there is only one functioning kidney which becomes obstructed, complete anuria may occur. More commonly partial obstruction can lead to renal impairment, despite continued passage of urine. Partial obstruction may also sometimes cause polyuria, due to loss of concentrating ability of the tubules.
┬Ę Acute obstruction is almost always associated with pain, but chronic progressive obstruction usually causes dilatation with little or no pain.
Clinical features
Renal obstruction should be considered as a diagnosis in all presentations of renal failure, as it is often asymptomatic. Loin pain, which may be dull, sharp, constant or intermittent, may occur. High intake of fluids may exacerbate the pain. Loin tenderness may be present, a distended bladder may be palpable and rectal and vaginal examination should be performed to look for pelvic disease.
Macroscopy
An acutely obstructed kidney is swollen, but chronic damage to the kidneys may make it small and shrivelled.
Complications
Infection above the level of obstruction can cause pyelonephritis (pyonephrosis is the term for an infected, obstructed hydronephrosis) or cystitis, and patients can become very unwell due to pain, fever and sepsis.
Investigations
The investigation of choice is a renal ultrasound (USS), as this will diagnose obstruction and its cause in most cases. If the kidneys are poorly visualised CT scanning is a useful substitute. In renal obstruction USS and CT will show a hydronephrosis, i.e. dilated renal pelvis and calyces (also called pelvicalyceal dilatation) and/or dilated ureters. However dilatation may not be seen if there is oligo-/anuria, in the first 72 hours before the systems have dilated, or if there is retroperitoneal fibrosis encasing the ureters. False positives may occur on USS or CT because of cysts, staghorn calculi or a dilated baggy low-pressure system, which may be mistaken for an obstructed system. Therefore, if there is doubt, one of the following may be required:
┬Ę Intravenous urogram (IVU). This is very useful, particularly in acute obstruction before there is dilatation, as it shows contrast ŌĆśheld upŌĆÖ by the obstruction and may show the lesion as a space-filling defect such as a radiolucent stone or a papilla. A plain film should be done first to look for radio-opaque stones. IVU should be avoided in renal failure.
┬Ę Radionuclide study such as MAG3 can show impaired uptake, delayed peak activity and delayed transit time on the side of the obstruction. This picture is also seen in any cause of renal impairment, but if it reverses with a dose of diuretics, then obstruction is not present.
┬Ę As part of the management percutaneous nephrostomy can be placed and then anterograde pyelography and ureterography can be performed through the nephrostomy. This avoids intravenous contrast. Alternatively retrograde ureterography can be performed, using a cystoscope. Catheters are introduced into the ureteric orifices and contrast injected. Cystoscopy may also visualise a cause of obstruction.
U&Es may demonstrate renal impairment. FBC may show a normochromic, normocytic anaemia of chronic disease.
Urine should be sent for microscopy and culture, urgently if infection is suspected.
Management
It is important to diagnose and treat urinary tract obstruction quickly, as delayed treatment can cause irreversible loss of renal function.
┬Ę Bladder catheterisation should be performed if bladder neck obstruction is suspected. Percutaneous nephrostomy is indicated for ureteric or pelviureteric junction obstruction. Acute renal failure and its complications require appropriate treatment.
┬Ę Infection of an obstructed system requires drainage of the system, together with high dose intravenous antibiotics.
┬Ę Relief of the obstruction can cause marked polyuria, as much as 500ŌĆō1000 mL/hour. Some of this is due to loss of concentrating ability of the tubules, which may take a few days to recover, but often the patient is also fluid overloaded. Careful fluid balance monitoring is needed, to avoid hypotension or prerenal failure during this phase.
Related Topics