Chapter: The Massage Connection ANATOMY AND PHYSIOLOGY : Skeletal System and Joints
The Pelvic Girdle
THE PELVIC GIRDLE
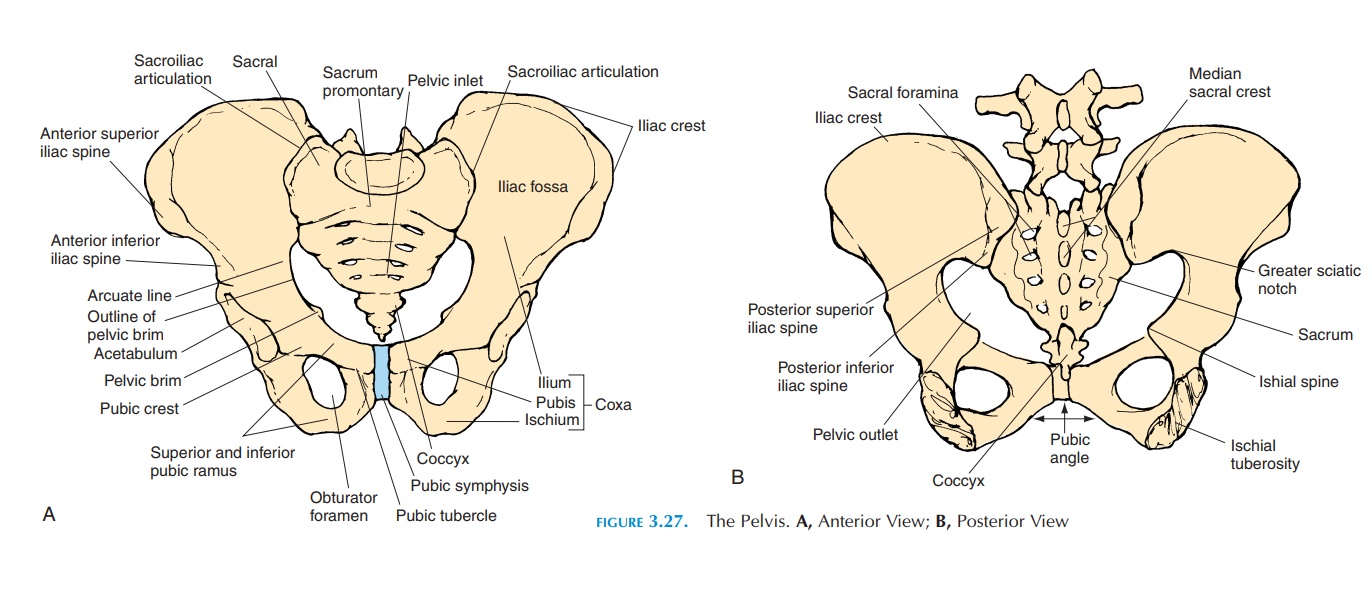
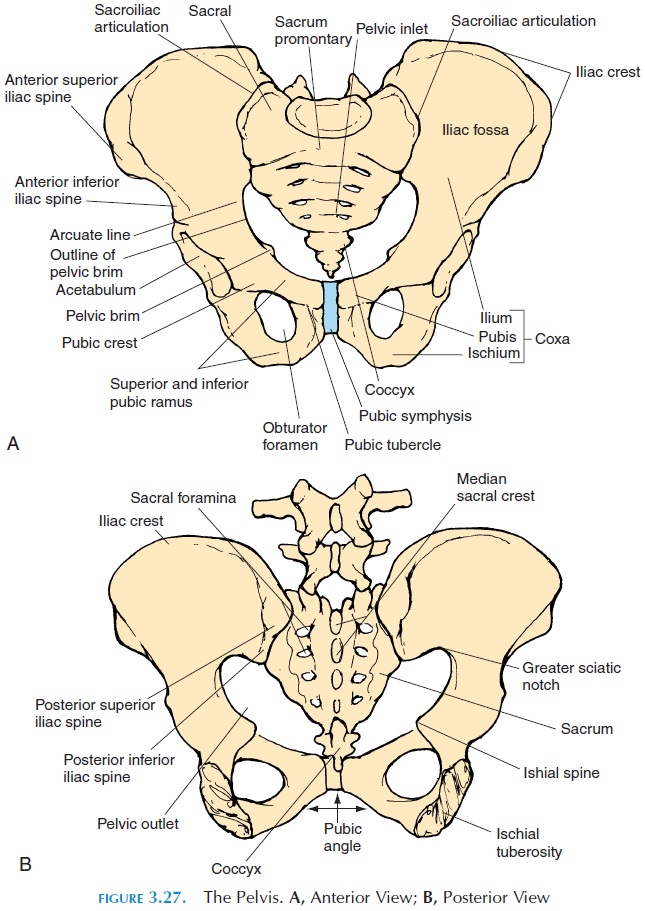
Each coxa, or hipbone (see Figure 3.27), is made of three bones that have fused together, the ilium, is-chium, and the pubis. The ilium articulates with thesacrum posteriorly and medially. On the lateral surface of the coxa, there is a rounded depression called the acetabulum. The femur articulates with the hipboneat the acetabulum. The three bones (ilium, ischium, and pubis) meet inside the acetabular fossa (the de-pression formed by the walls of the acetabulum).
Ilium
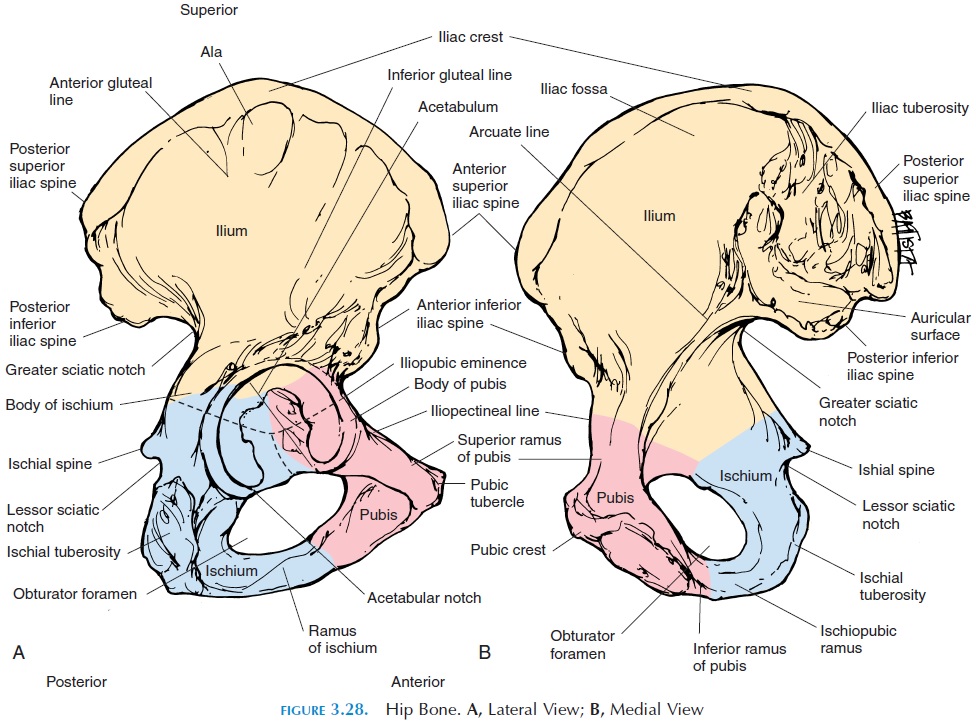
The ilium (see Figure 3.28) is the largest of the three bones and provides an extensive surface for attach-ment of muscles and tendons. It is in the form of a ridge superiorly, the iliac crest. Anteriorly, the iliac crest forms a prominence called the anterior supe-rior iliac spine. Posteriorly, the crest ends at the pos-terior superior iliac spine.Posteriorly and inferi-orly, there is a deep notch called the greater sciaticnotch. Other important landmarks on the ilium areshown in Figure 3.27.
Ischium
One important landmark on the ischium is the ischialspine—a projection just inferior to the greater sciaticnotch. The ischial tuberosity is the roughened pro-jection inferior to the ischial spine. This is the bone in your buttock that bears your weight when you sit. The ischium has a projection called the ischial ramus, which continues with the projection inferior ramus of the pubis. Together with the superior ramus of the pubis, the rami enclose an opening called the obtura-tor foramen. In life, this foramen is lined by connec-tive tissue that provides a base for attachment of mus-cles both on the interior and exterior surfaces. The medial surface of the pelvis has a shallow depression called the iliac fossa.
The pelvis is divided into the true (lesser) and the false (greater) pelvis. The true pelvis is the regionbelow an imaginary line that runs from the superior aspect of the sacrum to the superior margin of the pubic symphysis. The upper bony edge of the true pelvis is the pelvic brim and the opening is the pelvic inlet. When an obstetrician says that the headof the baby is fixed, it indicates that the head has en-tered the pelvic inlet.
The pelvic outlet is the opening bound by the in-ferior edges of the pelvis. This region is called the perineum in life and is bound by the coccyx, the is-chial tuberosities, and the inferior border of the pu-bic symphysis. Strong perineal muscles support the organs in the pelvic cavity.
Differences Between the Male and Female Pelvis
The male and female pelvis differs in shape and size. In females, the pelvis is lighter and smoother, with less prominent markings. The entire pelvis is low and broad. To facilitate childbearing, both the pelvic inlet and outlet are larger and wider in females. The arch made by the inferior rami of the pubis (pubic arch) is wider and the sacrum and coccyx are less curved, widening the pelvic outlet. Hormones secreted at pregnancy soften and loosen the ligaments and carti-lage in the pelvis, enabling the pelvis to widen fur-ther, if necessary, at delivery.
In females, the acetabulum is small and faces an-teriorly compared with that of males, where it is larger and faces laterally. This is partly responsible for the difference in gait between men and women. The shape of the obturator foramen is also different, being oval in females and round in males.
The Femur
The femur (see Figure 3.29) is the longest and heav-iest bone in the body. Proximally, it articulates with the pelvis and distally with the tibia at the knee joint. The superior aspect of the femur is rounded to form a head. The head narrows into a distinct neck that, in turn, joins with the shaft at an angle of about 125°. At the junction of the neck and shaft, a projec-tion is seen laterally. This is the greater trochanter. On the posteromedial surface, inferior to the greater trochanter, is the lesser trochanter. Anteriorly, a raised surface that runs between the greater and lesser trochanter, the intertrochanteric line, marks the point where the articular capsule of the hip joint is attached.
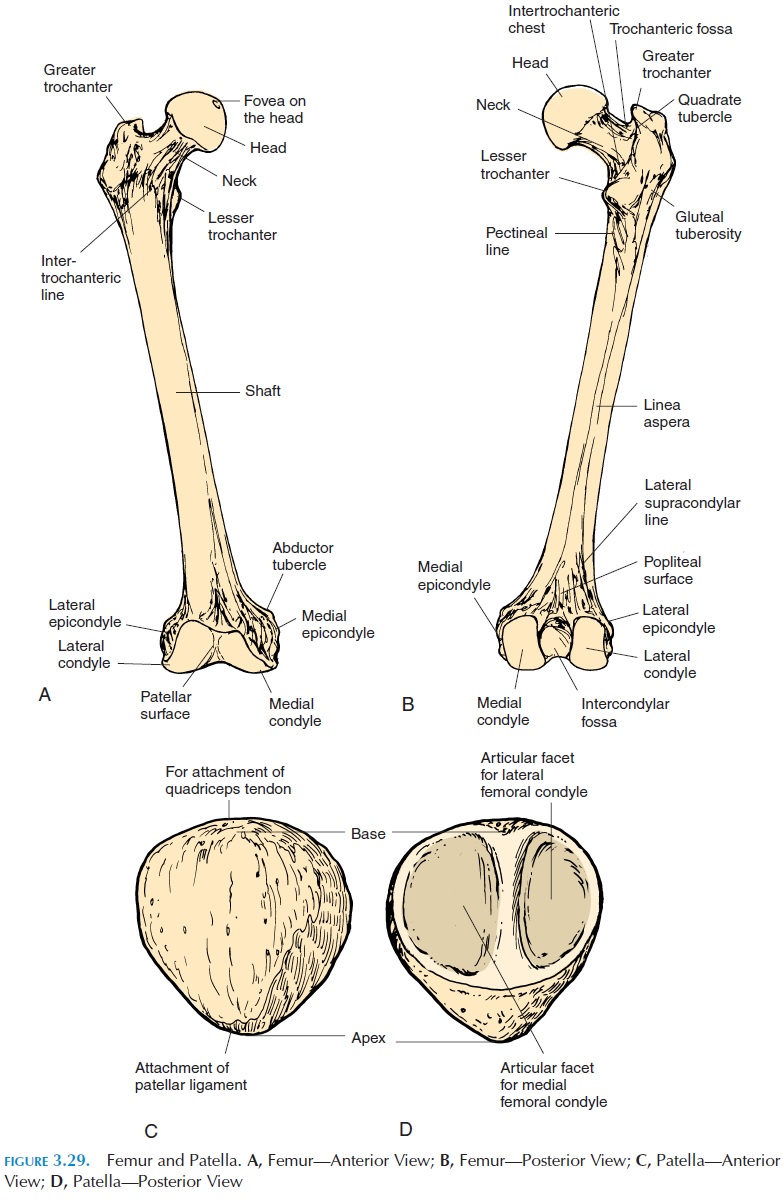
Along the posterior aspect of the shaft of the fe-mur, the linea aspera ridge runs down the center. Distally, the linea aspera divides into two ridges: the medial and thelateral supracondylar ridge. Thelower end of the femur widens into the medial and lateral condyles. The medial and lateral supra- condylar ridges end at roughened projections, the medial and lateral epicondyles, located on the me-dial and lateral condyles, respectively. A prominence just superior to the medial epicondyle, theadductortubercle, is where the tendon of the adductor mag-nus attaches. A deep depression, the intercondylarfossa, is seen between the condyles on the posteriorsurface of the lower end of the femur. Anteriorly, there is a smooth surface between the condyles. This is the surface that articulates with the patella, the patellar surface, or trochlear femoris.
The Patella
The patella (Figure 3.29C) is a large, triangular (with the apex pointing inferiorly) sesamoid bone, which is formed within the tendon of the quadriceps femoris muscle. The anterior, superior, and inferior surfaces are rough, indicating the regions that are attached to the ligaments and tendons. The anterior and inferior surface is attached to the patellar ligament, which con-nects the patella to the tibia. The anterior and superior surface is attached to the quadriceps tendon. The pos-terior surface is smooth, with a medial and lateral facet that articulates with the medial and lateral condyles of the femur.
The Tibia
The tibia (see Figure 3.30) is a large bone located me-dial to the fibula. The proximal end articulates with the condyles of the femur and the proximal end of the fibula. The distal end articulates with the tarsal bone—talus and the distal end of the fibula (laterally). The tibia and fibula, similar to the radius and ulna of the upper limb, are connected to each other by an in-terosseous membrane. The proximal, or upper end, is widened into a medial and lateral tibial condyle. A smaller projection, theintercondylar eminence, sep-arates the two condyles in the superior aspect of this widened end. The superior aspect that articulates with the condyles of the femur has amedial and lat-eral articular surface. Anteriorly, the proximal endhas a roughened area, the tibial tuberosity. This is where the patellar ligament is attached. Theanteriorcrest, or border, of the tibia is a ridge that runs infe-riorly, down the center of the tibia. This is the ridge that can be felt on the anterior aspect of the lower leg. Distally, too, the tibia widens to form projections. The large projection, the medial malleolus, is the bony prominence seen on the medial aspect of the ankle. It articulates with the talus. In the lateral aspect, the dis-tal end of the tibia articulates with the distal end of the fibula at the fibular notch.
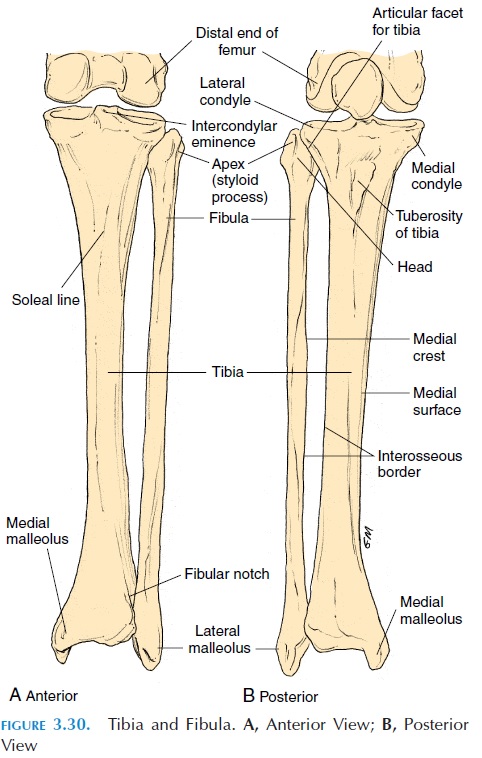
The Fibula
The fibula (Figure 3.30) is slender and is located lat-eral to the tibia. The proximal end is widened into the head. The head of the fibula articulates with thetibia, just inferior to the lateral condyle of the tibia. Along the shaft, a thin ridge, the interosseous crest, marks the surface that gives attachment to the strong connective tissueinterosseous membrane. The in-terosseous membrane bridges the gap between the tibia and the fibula along the two shafts, stabilizing the bones and increasing the anterior and posterior surface area for attachment of muscles. The lower end of the fibula widens to form a prominence called the lateral malleolus. The bony projection on the lateral aspect of the ankle is the lateral malleolus that articulates with the talus bone. Although the upper end of the fibula does not participate in the knee joint, the lower end is an important component of the ankle joint.
The Ankle
The ankle (tarsus) (see Figure 3.31) consists of the seven tarsal bones: the talus, calcaneus, cuboid,navicular, and the three cuneiforms.
The talus (Figure 3.31C) is the second largest of the tarsals and articulates with the lower end of the tibia and fibula. The superior, lateral, and medial sur-face of the talus appears smooth, as they are part of the ankle joint. The lateral surface has roughened surfaces that indicate the attachment of strong liga-ments that stabilize the joint.
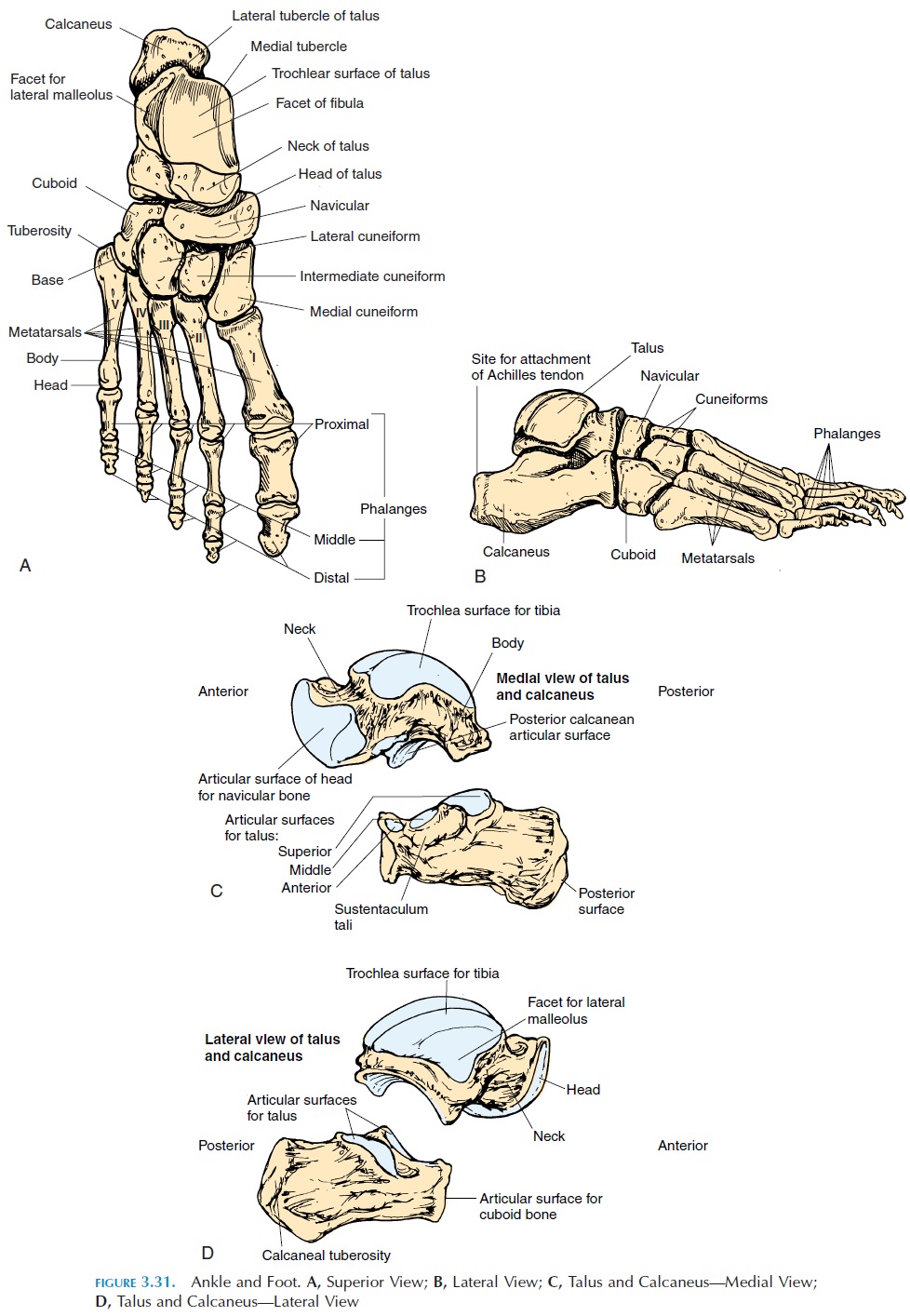
The heel bone, or the calcaneus, is the largest tarsal. The posterior surface of the calcaneus is rough-ened where the tendo calcaneus, or the Achilles ten-don, of the calf muscles is attached. Anteriorly and su-periorly, it is smooth where it articulates with the other tarsal bones. The cuboid and the cuneiforms ar-ticulate with the five metatarsals.
The five metatarsals form the bones of the sole of the foot. They are labeled I to V, proceeding medial to lateral (opposite that of the palm). Each metatarsal, like the metacarpals, has a base, body, and head. Dis-tally, the metatarsals articulate with the proximalphalanges. There are 14 phalanges—each toe hasthree, except for the great toe (hallux), which has two. As in the hand, the phalanges are named proxi-mal, middle, and distal phalanges, according to the position.
Related Topics