Chapter: Essentials of Psychiatry: Somatoform Disorders
Somatoform Disorders
Somatoform Disorders
Definition
The
somatoform disorders are a major diagnostic class in the Diagnostic and Statistical Manual
of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association,
2000) that groups together conditions characterized by physical symptoms
suggestive of but not fully explained by a general medical condition or the
direct effects of a substance. In this class, symptoms are not intentionally
produced and are not attributable to another mental disorder. To warrant a
diagnosis, symptoms must be clinically significant in terms of causing distress
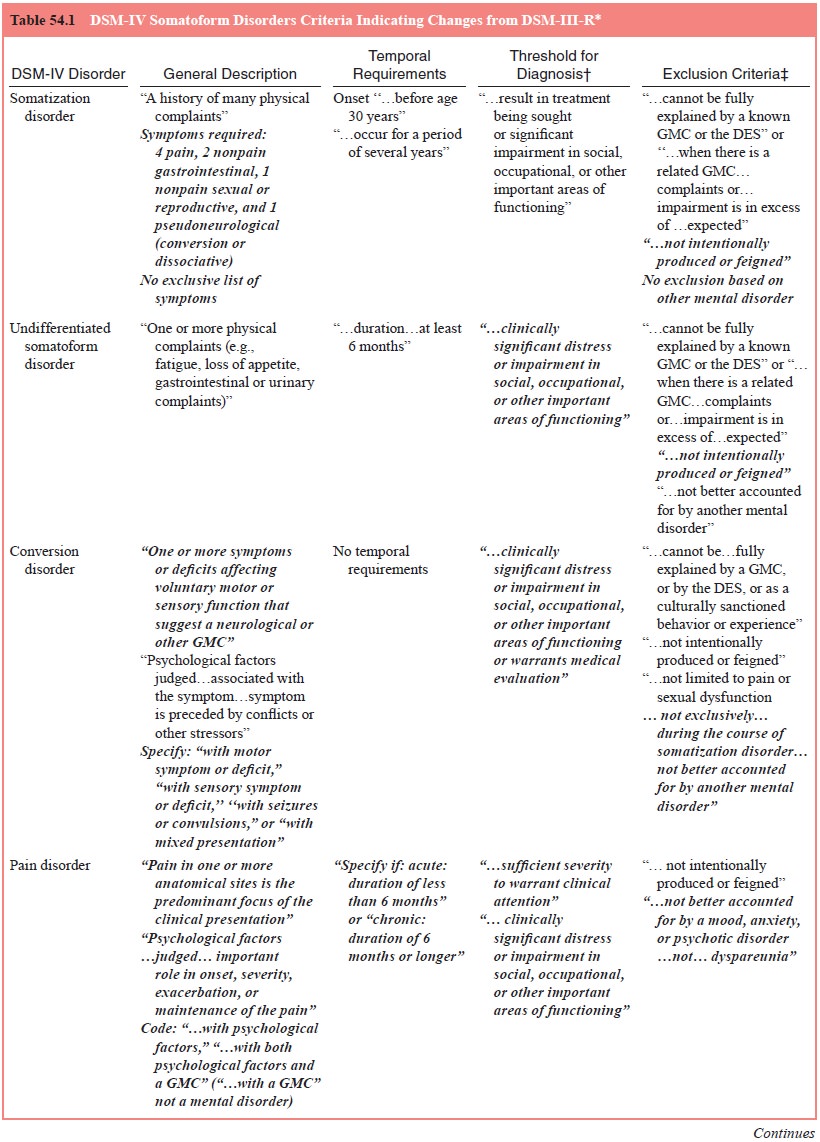
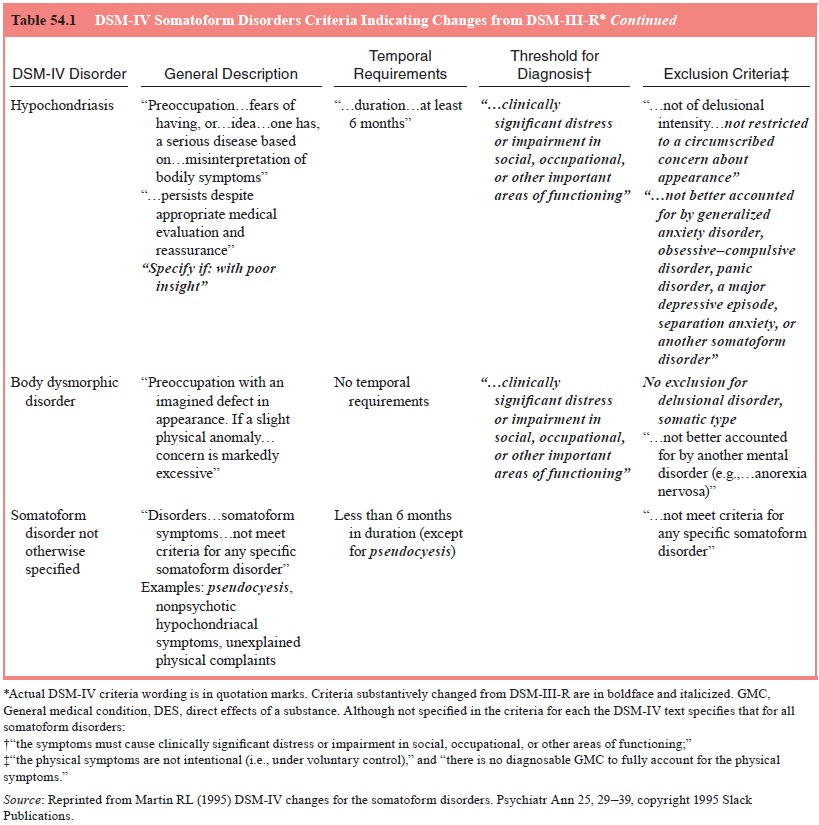
or impairment in important areas of functioning. As summarized in Table 54.1,
the disorders included in this class are somatization disorder,
undifferentiated somatoform disorder, conversion dis-order, pain disorder,
hypochondriasis, body dysmorphic disorder and somatoform disorder not otherwise
specified (NOS).
The somatoform disorders class was created for clinical utility, not on
the basis of an assumed common etiology or mech-anism. In DSM-IV-TR terms, it
was designed to facilitate the differential diagnosis of conditions in which
the first diagnostic concern is the need to “exclude occult general medical
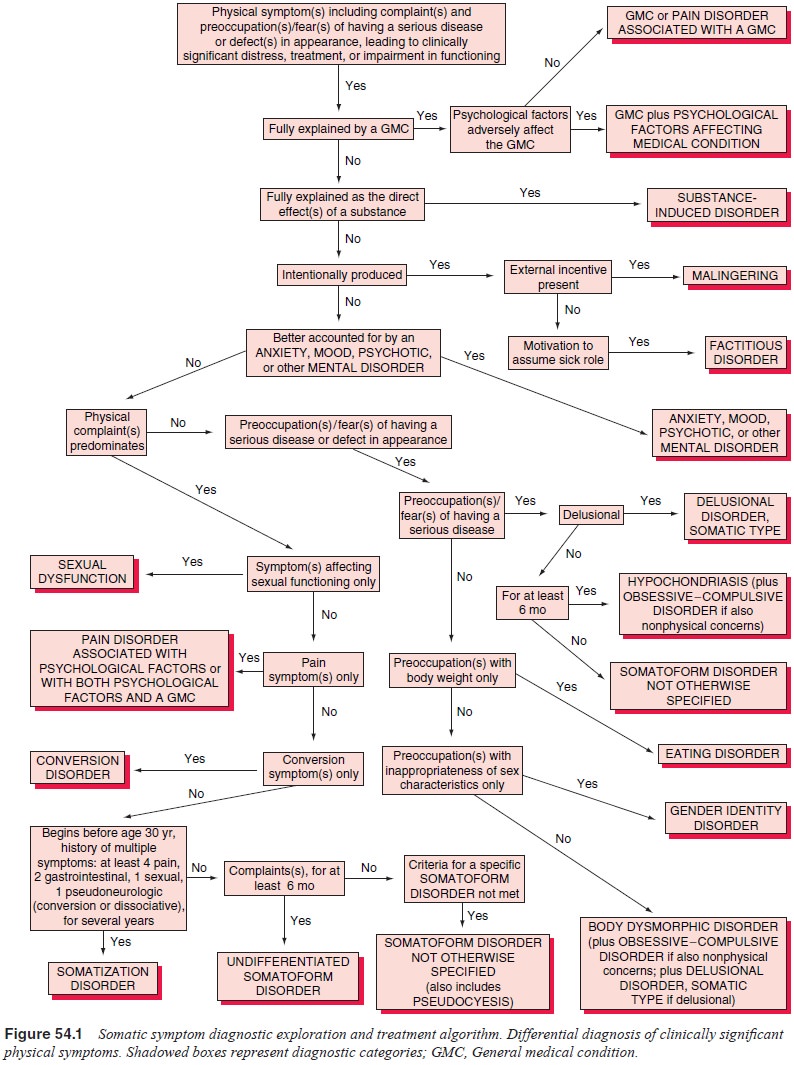
conditions or substance-induced etiologies for the bodily symptoms”. As shown
in Figure 54.1, only after such explanations are reasonably excluded should
somatoform disorders be considered.
Many criticisms of the somatoform disorder category have been raised and
they include contentions that because the category is delineated on the basis
of presenting symptoms, it is “superfi-cial”; that the individual disorders are
not qualitatively distinct from one another or from “normality” and hence would
be better described dimensionally rather than differentiated categorically;
that the disorders are derived from hospital rather than commu-nity- or primary
care-based populations; and, perhaps the most se-rious challenge, that the
grouping “gives the spurious impression of understanding”. On the other hand,
proponents maintain that the somatoform grouping represents a major advance
over previ-ous systems and that segregation of such disorders into a class has
helped clarify the conceptualization of the “mind–body” distinc-tion, promoted
greater consistency in terminology, and led to bet-ter descriptive distinctions
between specific disorders. Support-ers contend that maintaining this
diagnostic class will foster more generalizable and thereby more clinically
applicable research.
The somatoform disorder concept should be distin-guished from
traditional concepts of “psychosomatic illness” and “somatization”. The
psychosomatic illnesses involved structural or physiological changes
hypothesized as deriving from psychologi-cal factors. In the DSM-IV somatoform
disorders, such objective changes are generally not evident. The “classic”
psychosomatic illnesses of Alexander (1950) included bronchial asthma,
ulcerativecolitis, thyrotoxicosis, essential hypertension, rheumatoid
arthri-tis, neurodermatitis and peptic ulcer. In DSM-IV, most of these
ill-nesses would be diagnosed as a general medical condition on Axis III, and
in some cases with an additional designation of psychologi-cal factors
affecting medical condition on Axis I. By definition, the diagnosis of
“psychological factors affecting medical condition” is not a psychiatric
disorder, but it is included in DSM-IV in the sec-tion for other conditions
that may be a focus of clinical attention; it involves the presence of one or
more specific psychological or be-havioral factors that adversely affect a
general medical condition.
The descriptive use of the term “somatization” in somati-zation disorder
is not to be confused with theories that generally postulate a somatic
expression of psychological distress. Empirical studies suggest that there is
no single theory that can adequately explain somatization, which is not only
multifactorially deter-mined but is an exceedingly complex phenomenon.
Furthermore, treatment strategies derived from somatization theories have not
proven effective. For example, the postulation that patients with so-matoform
disorders are alexithymic, that is, are unable to process emotions and
psychological conflicts verbally and therefore do so somatically, suggested that
teaching such patients to “appreciate” and “verbalize” their emotions would
circumvent the need to “so-matize” them. Such treatment approaches have been
ineffective.
Related Topics