Chapter: Medicine Study Notes : Public Health
Social Inequalities in Health
Social Inequalities in Health
·
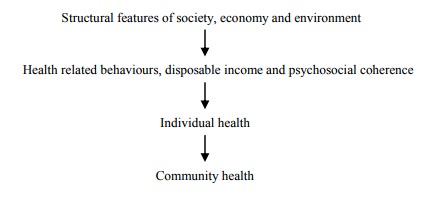
Deprived social and economic
conditions strongly associated with poor health
·
There is a social gradient in
health – it exists in all countries but the slope varies
·
Targets for intervention:
o Socio-economic status: issues around distribution
o Intermediary factors: housing, targeted support
o Health issues: access. Most
countries target their intervention here
o Link from Health to SES: disability support
·
Poor health ®
deprivation through stigma and ¯earning potential
·
Deprivation ® poor
health through the following:
Effect of Deprivation on Health
·
Poor access to health care:
o Culturally foreign
o Financial barriers: GP services, transport, class and language
differences between doctor and patient
·
Income:
o Key SES lever. Can have a rapid
effect on:
§ Effects of a drop in absolute income
§ Rise in income inequality ® divisive effect on society ® alienation of „work poor households‟:
· Measured by the Gini Co-efficient for household equivalent disposable income
·
Has for NZ
since 1988 from 0.26 to 0.33 (biggest change in the OECD)
· Is followed with a small lag by indicators such as youth suicide, youth unemployment, etc
§ Formation of social capital. People in „survival‟ mode don‟t have energy to contribute to community
o Policy levers: monitoring income inequality, change tax rates and social
wage, alter WINZ rules about supplements
o Single parent families, women, Maori and Pacific Islanders are over-represented in the poor
·
Education: Increases human
capital. Students from poor households are more likely to underachieve, have lower
participation rates in tertiary education.
·
Occupation and labour force
participation:
o Translates human capital into income.
Also indicator of social class
o Higher injury rates in low SES jobs (forestry, construction)
o Unemployment: stress, social isolation, lack of purpose ® ¯ self
esteem
· Housing:
o Impacts of rent, neighbourhood, number of bedrooms, quality of
construction and maintenance (eg insulation, ventilation).
o Issue for the poor, and also for former institutionalised psychiatric patients
o Damp housing ® respiratory illness, overcrowding ® infectious diseases, mental distress
· Feelings of hopelessness and being devalued ® less cohesive society ® violence, exploitation, drug use
·
Ethnicity:
o Interacts with SES
o Sensitive policy area
·
NZDep (NZ Deprivation Index) is a
composite measure of deprivation
·
Individual health risks:
o Adequate food in sufficient quantities („food security‟)
o Physical exercise: affected by range or sports facilities, clubs, etc
o Alcohol/tobacco consumption: affected by taxes, restrictions on
distribution
o Early pregnancy
o Also indicators such as obesity, high blood pressure, high cholesterol,
diet, exercise
·
Health behaviours/At-risk
behaviour (eg lifestyle factors)
o Health damaging behaviours more common in low SES
o Knowledge alone insufficient to change behaviour (eg smoking may be a coping strategy)
· Relate these factors to health status using measures of mortality, morbidity (including measurement of self-rated health status, suffer from specific diseases or measure role limitation), health risks, health service utilisation
·
NZ approach:
o Monitor social and economic determinants of health
o No systematic cross country comparisons
o Slow policy development and implementation
o Lacks cross party and public support
o Emphasis on health providers not determinants
·
Conclusions:
o Socio-economic determinants of health are multi-causal
o Issues around policy making under conditions of uncertainty
o Policies should be monitored against goals
Related Topics