Chapter: Basic & Clinical Pharmacology : Adrenocorticosteroids And Adrenocortical Antagonists
Selection of Drug & Dosage Schedule - Synthetic Corticosteroids
Selection of Drug & Dosage
Schedule
Glucocorticoid
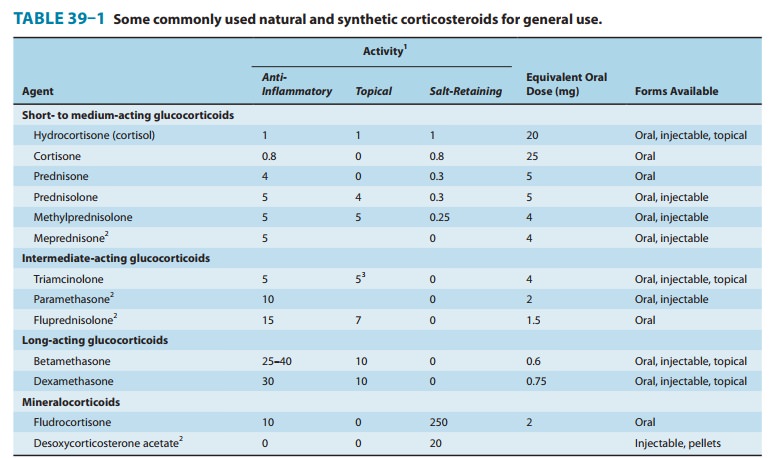
preparations differ with respect to relative anti-inflammatory and
mineralocorticoid effect, duration of action, cost, and dosage forms available
(Table 39–1), and these factors should be taken into account in selecting the
drug to be used.
A. ACTH versus Adrenocortical Steroids
In patients with
normal adrenals, ACTH was used in the past to induce the endogenous production
of cortisol to obtain similar effects. However, except when an increase in
androgens is desir-able, the use of ACTH as a therapeutic agent has been
abandoned. Instances in which ACTH was claimed to be more effective than
glucocorticoids were probably due to the administration of smaller amounts of
corticosteroids than were produced by the dosage of ACTH.
B. Dosage
In determining the
dosage regimen to be used, the physician must consider the seriousness of the
disease, the amount of drug likely to be required to obtain the desired effect,
and the duration of therapy. In some diseases, the amount required for
maintenance of the desired therapeutic effect is less than the dose needed to
obtain the initial effect, and the lowest possible dosage for the needed effect
should be determined by gradually lowering the dose until a small increase in
signs or symptoms is noted.
When it is necessary
to maintain continuously elevated plasma corticosteroid levels to suppress
ACTH, a slowly absorbed paren-teral preparation or small oral doses at frequent
intervals are required. The opposite situation exists with respect to the use
of corticosteroids in the treatment of inflammatory and allergic dis-orders.
The same total quantity given in a few doses may be more effective than that
given in many smaller doses or in a slowly absorbed parenteral form.
Severe autoimmune
conditions involving vital organs must be treated aggressively, and
undertreatment is as dangerous as over-treatment. To minimize the deposition of
immune complexes and the influx of leukocytes and macrophages, 1 mg/kg/d of
prednisone in divided doses is required initially. This dosage is main-tained
until the serious manifestations respond. The dosage can then be gradually
reduced.
When large doses are
required for prolonged periods of time, alternate-day administration of the
compound may be tried after control is achieved. When used in this manner, very
large amounts (eg, 100 mg of prednisone) can sometimes be administered with
less marked adverse effects because there is a recovery period between each
dose. The transition to an alternate-day schedule can be made after the disease
process is under control. It should be done gradu-ally and with additional
supportive measures between doses.
When selecting a drug
for use in large doses, a medium- or intermediate-acting synthetic steroid with
little mineralocorticoid effect is advisable. If possible, it should be given
as a single morning dose.
C. Special Dosage Forms
Local therapy, such as
topical preparations for skin disease, oph-thalmic forms for eye disease,
intra-articular injections for joint disease, inhaled steroids for asthma, and
hydrocortisone enemas for ulcerative colitis, provides a means of delivering
large amounts of steroid to the diseased tissue with reduced systemic effects.
Beclomethasone
dipropionate, and several other glucocorti-coids—primarily budesonide,
flunisolide, and mometasone furoate, administered as aerosols—have been found
to be extremely useful in the treatment of asthma .
Beclomethasone
dipropionate, triamcinolone acetonide, budes-onide, flunisolide, and mometasone
furoate are available as nasal sprays for the topical treatment of allergic
rhinitis. They are effec-tive at doses (one or two sprays one, two, or three
times daily) that in most patients result in plasma levels that are too low to
influ-ence adrenal function or have any other systemic effects.
Corticosteroids incorporated in ointments, creams, lotions, and sprays are used extensively in dermatology.
Related Topics