Chapter: Clinical Anesthesiology: Anesthetic Management: Obstetric Anesthesia
Regional Anesthetic Techniques: Spinal Opioids Alone
REGIONAL ANESTHETIC TECHNIQUES
Epidural or intrathecal techniques, alone or
in com-bination, are currently the most popular methods of pain relief during
labor and delivery. They can pro-vide excellent analgesia while allowing the
mother to be awake and cooperative during labor. Although spinal opioids or
local anesthetics alone can provide satisfactory analgesia, techniques that
combine the two have proved to be the most satisfactory in mos parturients.
Moreover, the synergy between opioids and local anesthetics decreases doserequirements
and provides excellent analgesia with few maternal side effects and little or
no neonatal depression.
Spinal
Opioids Alone
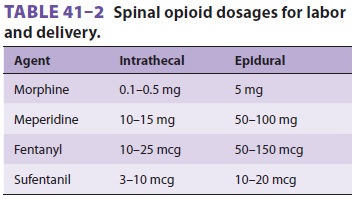
Opioids may be given intrathecally as a
single injec-tion or intermittently via an epidural or intrathe-cal catheter (Table
41–2). Relatively large doses are required for
analgesia during labor when epidural or intrathecal opioids are used alone. For
example, the ED50
during labor is 124 mcg for epidural fentanyl and 21 mcg for epidural
sufentanil. The higher doses may be associated with a high risk of side ef
fects, most importantly respiratory depression. For that reason combinations of
local anesthetics and opioids are most commonly used . Pure opioid techniques
are most useful for high-risk patients who may not tolerate the functional
sympathec-tomy associated with spinal or epidural anesthesia . This group
includes patients with hypovolemia or significant cardiovascular disease such
as moderate to severe aortic stenosis, tetralogy of Fallot, Eisenmenger’s
syndrome, or pulmonary hypertension. With the exception of meperidine, which
has local anesthetic properties, spinal opi-oids alone do not produce motor
blockade or sym-pathectomy. Thus, they do not impair the ability of the
parturient to “push.” Disadvantages include
less complete analgesia, lack of perineal relaxation, and side effects
such as pruritus, nausea, vomiting, sedation, and respiratory depression. Side
effects may be ameliorated with low doses of naloxone (0.1–0.2 mg/h
intravenously).
Intrathecal Opioids
Intrathecal morphine in doses of 0.1–0.5 mg may produce satisfactory and
prolonged (4–6 h) anal-gesia during the first stage of labor. Unfortunately,
the onset of analgesia is slow (45–60 min), and these doses may not be
sufficient in many patients. Higher doses are associated with a relatively high
incidence of side effects. Morphine is therefore rarely used alone. The
combination of morphine, 0.1–0.25 mg, and fentanyl, 12.5 mcg (or sufentanil, 5
mcg), may result in a more rapid onset of analgesia (5 min). Intermittent
boluses of 10–15 mg of meperidine, 12.5–25 mcg of fentanyl, or 3–10 mcg of
sufentanil via an intrathecal catheter can also provide satisfac-tory analgesia
for labor. Early reports of fetal bra-dycardia following intrathecal opioid
injections (eg, sufentanil) have not been confirmed by subsequent studies.
Hypotension following administration of intrathecal opioids for labor is likely
related to the resultant analgesia and decreased circulating cat-echolamine
levels.
Epidural Opioids
Relatively large doses (≥7.5 mg) of epidural
mor-phine are required for satisfactory labor analgesia, but doses larger than
5 mg are not recommended because of the increased risk of delayed respiratory
depression and because the resultant analgesia is effective only in the early
first stage of labor. Onset may take 30–60 min but analgesia lasts up to 12–24
h (as does the risk of delayed respiratory depression). Epidural meperidine,
50–100 mg, provides good, but relatively brief, analgesia (1–3 h). Epidural
fen-tanyl, 50–150 mcg, or sufentanil, 10–20 mcg, usu-ally produces analgesia
within 5–10 min with few side effects, but it has a short duration (1–2 h).
Although “single-shot” epidural opioids do not appear to cause significant
neonatal depression, caution should be exercised following repeated
administrations. Combinations of a lower dose of morphine, 2.5 mg, with
fentanyl, 25–50 mcg (or sufentanil, 7.5–10 mcg), may result in a more
rapid onset and prolongation of analgesia (4–5 h) with fewer side effects.
Related Topics