Chapter: Clinical Dermatology: Psoriasis
Psoriasis: Presentation
Presentation
Common patterns
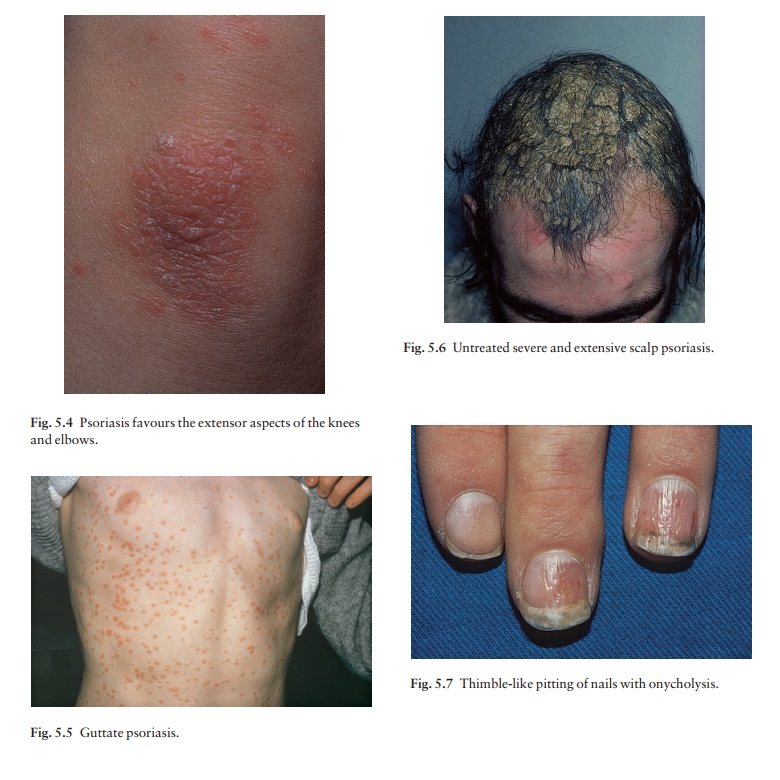
Plaque pattern
This
is the most common type. Lesions are well demarcated and range from a few
millimetres to several centimetres in diameter (Fig. 5.3). The lesions are pink
or red with large dry silvery-white polygonal scales (like candle grease). The
elbows, knees, lower back and scalp are sites of predilection (Fig. 5.4).


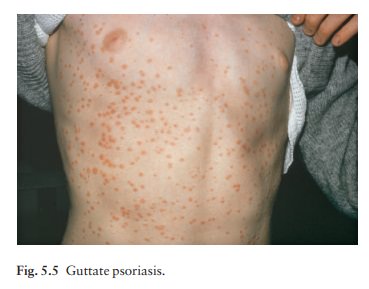
Guttate pattern
This
is usually seen in children and adolescents and may be the first sign of the
disease, often trig-gered by streptococcal tonsillitis. Numerous small round
red macules come up suddenly on the trunk and soon become scaly (Fig. 5.5). The
rash often clears in a few months but plaque psoriasis may develop later.
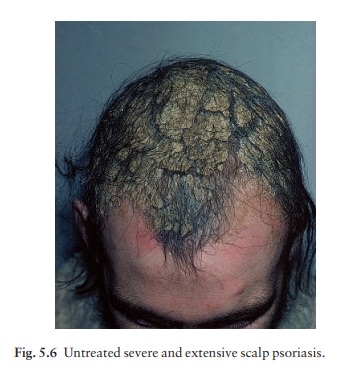
Scalp
The
scalp is often involved. Areas of scaling are inter-spersed with normal skin;
their lumpiness is more easily felt than seen (Fig. 5.6). Frequently, the
psoriasis overflows just beyond the scalp margin. Significant hair loss is
rare.
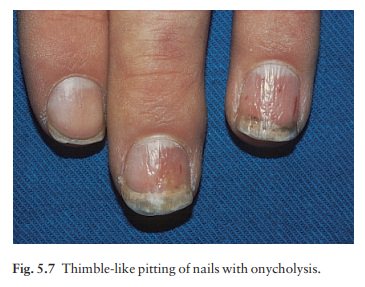
Nails
Involvement of the nails is common, with ‘thimble pitting’ (Fig. 5.7), onycholysis (separation of the nail from the nail bed; Fig. 5.8) and sometimes subungual hyperkeratosis.

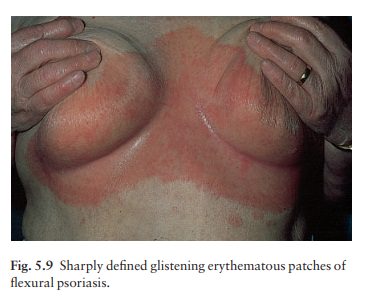
Flexures
Psoriasis
of the submammary, axillary and anogenital folds is not scaly although the
glistening sharply demarcated red plaques (Fig. 5.9), often with fissuring in
the depth of the fold, are still readily recognizable. Flexural psoriasis is
most common in women and in the elderly, and is more common among HIV-infected
individuals than uninfected ones.
Palms and soles
Palmar
psoriasis may be hard to recognize as its lesions are often poorly demarcated
and barely erythematous. The fingers may develop painful fissures.
Less common patterns
Napkin psoriasis
A psoriasiform spread outside the napkin (nappy/ diaper) area may give the first clue to a psoriatic tendency in an infant (Fig. 5.10). Usually it clears quickly but there is an increased risk of ordinary psoriasis developing in later life.

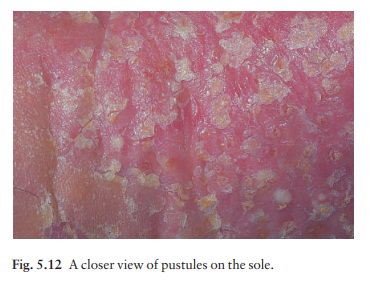
Localized pustular psoriasis (palmo-plantar pustulosis)
This
is a recalcitrant, often painful condition which some regard as a separate
entity. It affects the palms and soles, which become studded with numerous
sterile pustules, 3–10 mm in diameter, lying on an erythematous base. The
pustules change to brown macules or scales (Figs 5.11 and 5.12). Generalized
pustular psoriasis is a rare but serious condition, with fever and recurrent
episodes of pustulation within areas of erythema.

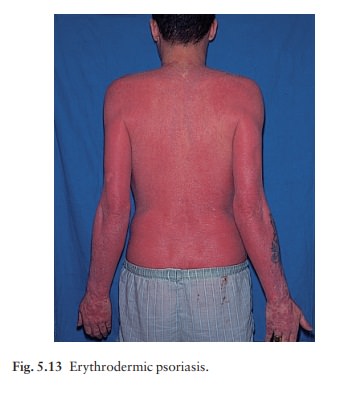
Erythrodermic psoriasis
This
is also rare and can be sparked off by the irritant effect of tar or dithranol,
by a drug eruption or by the withdrawal of potent topical or systemic steroids.
The skin becomes universally and uniformly red with variable scaling (Fig.
5.13). Malaise is accompanied by shivering and the skin feels hot and
uncomfortable.
Related Topics