Chapter: Clinical Anesthesiology: Anesthetic Management: Maternal & Fetal Physiology & Anesthesia
Physiological Transition of the Fetus at Birth
PHYSIOLOGICAL TRANSITION OF THE FETUS AT BIRTH
The most profound adaptive changes at birth involve the circulatory and respiratory
systems. Failure to make this transition successfully results in fetal death or
permanent neurological damage.
At term, the fetal lungs are developed but
contain about 90 mL of a plasma ultrafiltrate. During expul-sion of the fetus
at delivery, this fluid is normally squeezed from the lungs by the forces of
the pelvic muscles and the vagina acting on the baby (the vagi-nal squeeze).
Any remaining fluid is reabsorbed by the pulmonary capillaries and lymphatics.
Small (pre-term) neonates and neonates delivered via cesarean section do not
benefit from the vaginal squeeze and thus typically have greater difficulty in
maintaining respirations (transient tachypnea of the newborn). Respiratory
efforts are normally initiated within 30 s after birth and become sustained
within 90 s. Mild hypoxia and acidosis as well as sensory stimulation— cord
clamping, pain, touch, and noise—help initiate and sustain respirations,
whereas the outward recoil of the chest at delivery aids in filling the lungs
with air.
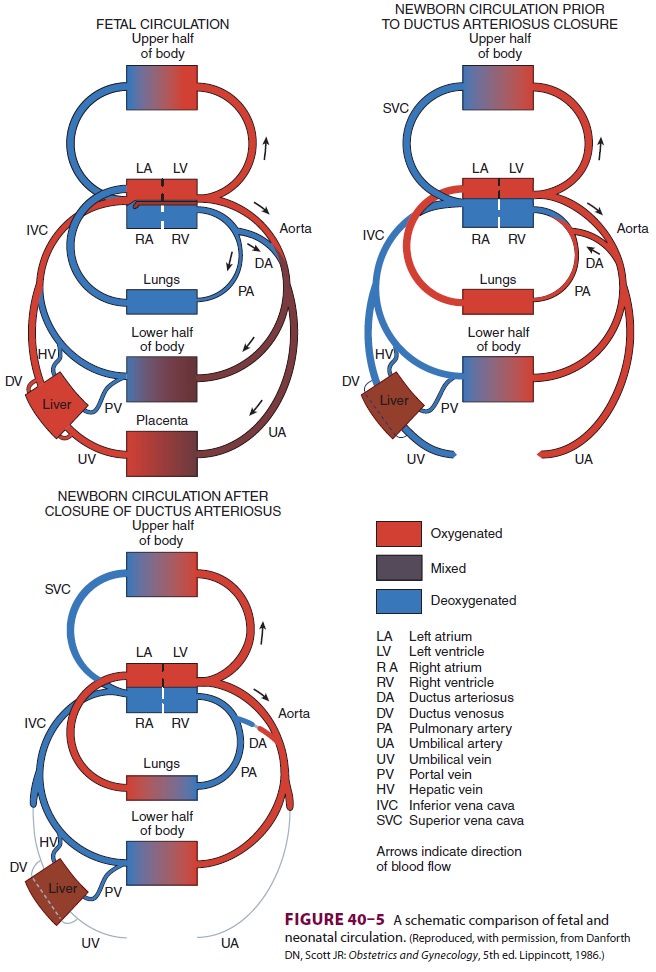
Lung expansion increases both alveolar and
arterial oxygen tensions and decreases pulmonary vascular resistance. The
increase in oxygen tension is a potent stimulus for pulmonary arterial
vasodi-lation. The resultant increase in pulmonary blood flow and augmented
flow to the left heart elevates left atrial pressure and functionally closes
the fora-men ovale. The increase in arterial oxygen tension also causes the
ductus arteriosus to contract and functionally close. Other chemical mediators
that may play a role in ductal closure include acetylcho-line, bradykinin, and
prostaglandins. The overall result is elimination of right-to-left shunting and
establishment of the adult circulation (Figure 40–5). Anatomic closure of the
ductus arteriosus does not usually occur until about 2–3 weeks, whereas closure
of the foramen ovale takes months if it occurs at all.
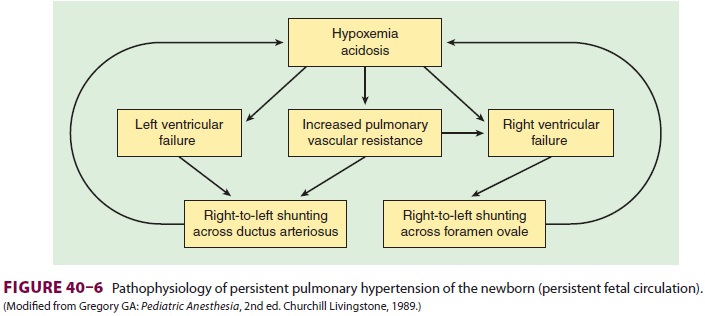
Hypoxia or acidosis during the first few days
of life can prevent or reverse these physiological changes, resulting in
persistence of (or return to) the fetal circulation, or persistent pulmonary
hyper-tension of the newborn. A vicious circle is estab-lished where the
right-to-left shunting promotes hypoxemia and acidosis, which in turn promote
more shunting (Figure 40–6). Right-to-left
shunting may occur across the foramen ovale, the ductus arte-riosus, or both.
Unless this circle is broken, neonatal demise can occur rapidly.
Related Topics