Chapter: Basic & Clinical Pharmacology : Introduction to Autonomic Pharmacology
Pharmacologic Modification of Autonomic Function
PHARMACOLOGIC MODIFICATION OF
AUTONOMIC FUNCTION
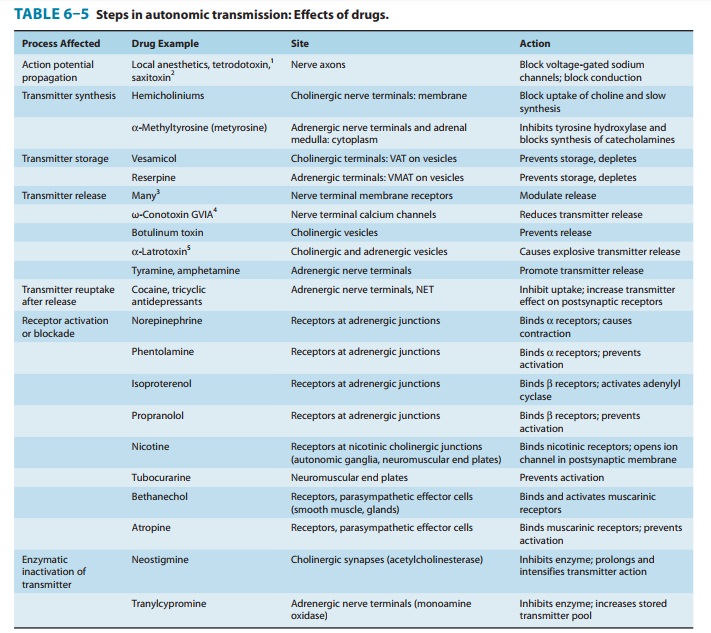
Because transmission involves different mechanisms in differ-ent segments of the ANS, some drugs produce highly specific effects, whereas others are much less selective in their actions. A summary of the steps in transmission of impulses, from the CNS to the autonomic effector cells, is presented in Table 6–5. Drugs that block action potential propagation (local anesthetics and some natural toxins) are very nonselective in their action, since they act on a process that is common to all neurons. On the other hand, drugs that act on the biochemical processes involved in transmitter synthesis and storage are more selective, since the biochemistry of each transmitter differs, eg, norepi-nephrine synthesis is very different from acetylcholine synthesis. Activation or blockade of effector cell receptors offers maximum flexibility and selectivity of effect attainable with currently available drugs: adrenoceptors are easily distinguished from cholinoceptors.
Furthermore,
individual receptor subgroups can often be selectively activated or blocked
within each major type. Some examples are given in the Box: Pharmacology of the
Eye.
Even greater selectivity may be attainable in the future using drugs that
target post-traditional receptor processes, eg, receptors for second
messengers.
Pharmacology of the Eye
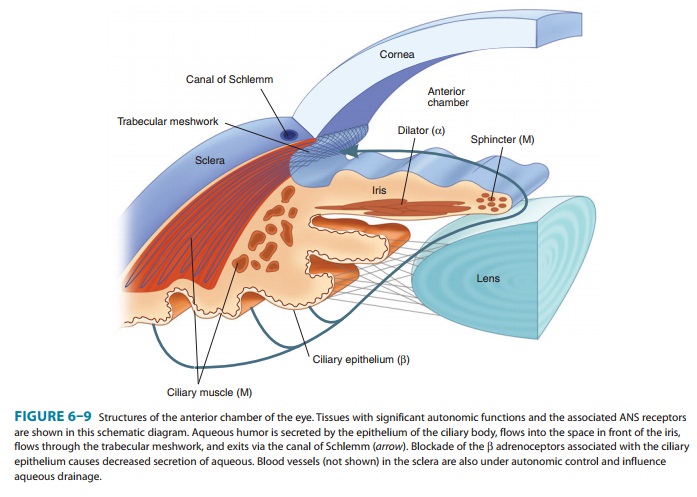
The eye is
a good example of an organ with multiple autonomic functions, controlled by several
autonomic receptors. As shown in Figure 6–9, the anterior chamber is the site
of several autonomic effector tissues. These tissues include three muscles
(pupillary dila-tor and constrictor muscles in the iris and the ciliary muscle)
and the secretory epithelium of the ciliary body.Parasympathetic nerve activity
and muscarinic cholinomimet-ics mediate contraction of the circular pupillary
constrictor muscle and of the ciliary muscle. Contraction of the pupillary
constrictor muscle causes miosis, a reduction in pupil size. Miosis is usually
present in patients exposed to large systemic or small topical doses of
cholinomimetics, especially organophosphate cholinest-erase inhibitors. Ciliary
muscle contraction causes accommoda-tion of focus for near vision. Marked
contraction of the ciliary muscle, which often occurs with cholinesterase
inhibitor intoxication, is called cyclospasm. Ciliary muscle contraction also
puts tension on the trabecular meshwork, opening its pores and facilitating
outflow of the aqueous humor into the canal of Schlemm. Increased outflow
reduces intraocular pressure, a very useful result in patients with glaucoma.
All of these effects are prevented or reversed by muscarinic blocking drugs
such as atropine.
Alpha
adrenoceptors mediate contraction of the radially ori-ented pupillary dilator
muscle fibers in the iris and result in mydriasis. This occurs during
sympathetic discharge and when α-agonist drugs such as phenylephrine are placed
in the conjunc-tival sac. Beta adrenoceptors on the ciliary epithelium
facilitate the secretion of aqueous humor. Blocking these receptors (with
β-blocking drugs) reduces the secretory activity and reduces intraocular
pressure, providing another therapy for glaucoma.
Related Topics