Chapter: Forensic Medicine: Toxicology and alcohol
Pharmacodynamics of alcohol
Pharmacodynamics of alcohol
Pharmacodynamics is the study of the action of
drugs on living organisms. Although alcohol may be theoretically introduced
into the body via the rectum, intravenously or even by inhalation, the most
common, and for all practical purposes the only, route is by ingestion.
Absorption of alcohol by the body
a Ingestion of alcohol
Alcohol is usually taken by mouth in one or
other form and is absorbed into the body directly and unchanged by the process
of diffusion. Alcohol, unlike other substances like sugars, is not chemically
modified in any way before it is absorbed. The process of diffusion occurs
through the mucous membranes (ie the membranes coating the inner surface of the
stomach, intestines, etc) into the large network of capillary blood vessels in
the alimentary canal.
The absorption of alcohol in the mouth and
oesophagus is minimal and for practical purposes nil, because the alcohol
passes rapidly through these structures. Absorption proceeds immediately in the
stomach and small intestine. Approximately 20% of alcohol which is ingested is
absorbed in the stomach, and the rest (80%) in the small intestine. Depending
on the volume of alcohol ingested, a small quantity may reach the colon and be
absorbed there. If alcohol is administered into the colon by means of an enema,
the absorption there is also rapid and complete.
i Anatomical and physical factors of importance
Alcohol absorbed by the stomach and small
intestine is first absorbed into the blood and then distributed to all the
organs. The following anatomical and physical factors determine not only the
rate of absorption, but also the site of maximum absorption:
Surface of the mucous membrane
Due to its length the small intestine has a far
greater surface area of mucous membrane than the stomach. Thus alcohol is
absorbed much faster from the small intestine than from the stomach. If the
mucous membrane is covered by mucus or food this will delay the absorption
because the area of contact between the alcohol and the mucous membrane is
less.
Absorption capacity of the mucous membrane
The mucous membrane of the small intestine has a
better supply of blood vessels than that of the stomach, and therefore
absorption in the small intestine is greater than in the stomach. Any condition
which increases the blood supply in the mucous membrane will increase absorption,
for example congestion and/or gastritis or dilatation of the capillaries by
warm or hot liquids. The rate of absorption (diffusion) of alcohol depends on
the concentration gradient between the alcohol in the stomach and the
intestine, and the alcohol in the blood of the capillaries in the stomach and
intestinal wall. The smaller the gradient, the slower the rate of absorption
(Fick's law).
ii Factors influencing the rate of alcohol absorption
Using the above information as background it is
possible to classify the relevant factors. We discuss them in some detail.
The peristaltic movement of the alimentary canal and the functional
status of the stomach's pyloric sphincter. The forward propulsion of food is due to
rhythmic contractions called peristaltic movements or peristalsis. A muscle
forming a valve, the pyloric sphincter, is present at the stomach outlet. It is
this valve which controls the flow of food out of the stomach and into the
small intestine. Any condition which stimulates contraction of this valve will
therefore slow down the rate of forward movement of food (and alcohol).
The greater the gastric motility and the more
relaxed the pyloric sphincter, the more rapid the absorption of alcohol because
the gastric contents (mixed with alcohol) pass more rapidly into the duodenum
(the first part of the small intestine). Gastric motility is decreased by
certain medicines, by very high alcohol concentrations (paralysis of the smooth
muscle of the gastric wall) and in cases of nausea and shock. Gastric motility
is increased by the intake of large volumes of food and/or liquids. The rate at
which the stomach is emptied is increased by conditions of inflammation such as
peptic ulcers, as these cause gastric irritation.
Irritating substances in the stomach cause the
pyloric sphincter to contract and there is then a delay in the emptying of the
stomach. Psychological factors such as anxiety may influence the function of
the pyloric sphincter, but it is not possible to predict whether more or less
alcohol will then be absorbed because this differs from person to person.
Surgical procedures of the stomach and the small
intestine (eggastrectomy) will cause more rapid absorption of alcohol as the
gastric contents will pass more rapidly into the small intestine.
Thus, if the gastric contents are slowly
released into the small intestine, absorption will be slower and over a longer
period. Therefore the blood-alcohol level will not rise so high because the
body will have more time to eliminate the alcohol already absorbed, in other
words, it will be more able to cope with the absorbed alcohol.
The nature, composition, amount and strength of the beverage ingested. Optimal absorption of alcohol occurs when the
beverage has an alcohol concentration of between 10% and 20%. The higher the
concentration, the slower the absorption, because of the possible secretion of
excessive mucus, spasm of the pyloric sphincter and/or suppression of gastric
motility. Large volumes of beverage make contact with the mucous membranes over
a larger area and also increase the gastric motility so that alcohol passes
more rapidly into the small intestine. Absorption of the alcohol in beer is
delayed because of the presence of carbohydrates in the beer. The alcohol in
beverages that contain gas or to which diluents containing gas (carbon dioxide,
bicarbonate) have been added, is absorbed faster. This is due to the distension
of the stomach with gas, and therefore increasing the surface contact area due
to flattening of the normal stomach folds, almost similar to an inflated
balloon.
Warm beverages are absorbed faster than cold
ones and hence also the alcohol in the beverage. This is due to an increase in
the blood flow to the intestines.
To summarise: the most ``potent'' drink (if
someone is crazy enough to drink it) will be a warm bottle of champagne (warm - absorbed faster than cold; bottle - large volume; champagne - contains gas and has an alcohol concentration
between 10% and 20%)!
The contents of the alimentary canal. The absorption of alcohol from the stomach and
small intestine is influenced by the nature and amount of their contents. Food
``dilutes'' alcohol and prevents contact between the alcohol and the mucous
membrane. This is especially true of fatty foods and/or food with a high
protein and/or carbohydrate (sugar) content. Certain foods, especially fats,
delay the emptying of the stomach so that the food-alcohol mixture takes longer
to reach the small intestine with its large absorptive surface. It therefore
makes good sense not to drink on an empty stomach.
Medicines and other chemical substances. As mentioned above, various substances influence
gastric and intestinal peristalsis and the activity of the pyloric sphincter,
thus influencing the speed of absorption. This is a specialised field, and
often used in courts as a line of defence; for this course it is sufficient to
be aware of the possible role pharmaceutical substances may play.
b Absorption through the airways and lungs
Although absorption through the airways and
lungs can be rapid, it is highly unlikely that significant blood concentrations
will be reached, as the alcohol irritates the airways. The maximum blood
concentration reached through inhalation is 0,02g%. People do not die of
alcohol intoxication when they enter a wine tank, but they die of anoxia
(absence of oxygen) or the accumulation of carbon dioxide (CO2).
c Absorption through the skin
Alcohol is not absorbed through an intact skin.
d Intravenous and subcutaneous administration
This route is theoretically possible.
There is common misconception that the clinical
effect of alcohol intoxication is determined by the rate of absorption of
alcohol. This is wrong; a specific alcohol level will correspond with a
specific clinical effect, regardless of how rapidly that level was reached.
Distribution
After absorption from the gastro-intestinal
system, alcohol is distributed through the body via the blood circulation.
Certain factors will affect the distribution:
a Cardiac output
Any increase in cardiac output, such as caused
by exercise or excitement, will increase distribution.
b Water in tissues
Alcohol is water soluble. The water in an organ
or tissue will therefore determine the amount of alcohol which can dissolve in
that specific tissue. In tissues with a high water content more alcohol can
dissolve. Males have (supposedly) a higher muscle mass than females; the latter
have a higher fat content. Therefore males can redistribute more alcohol out of
their blood into their extra-vascular areas (muscles). That is why, all other
factors being equal, a male will have a lower blood-alcohol level than an
identical female counterpart after absorption of the same amount of alcohol.
This factor is also called the distribution factor or ``r'' factor in the
Widmark formula (0,7 for males and 0,6 for females).
c General
Alcohol does not accumulate in any organ or
tissue. If the blood-alcohol level drops below the alcohol level in the tissues
(brain or muscles), alcohol will diffuse from the tissues (higher
concentration) to the blood (lower concentration). This enables the body to
eventually get rid of all the absorbed alcohol.
Metabolism and secretion of alcohol
About 85% to 90% of alcohol is metabolised by
the liver. The enzyme, alcoholdehydrogenase (ADH), plays a major role in this
process. The metabolites produced by this process include acetaldehyde, one of
the causes of a hangover. The rest is secreted unchanged via the lungs, kidneys
and perspiration. Alcohol is eliminated at a constant rate. The rate of
elimination is between 0,01 and 0,02g% per hour. Usually the average (0,015g%
per hour) is used, and this is called the B60 value.
The elimination rate is more or less constant
for a given individual and is not affected by cold, exercise, sleep or any
other factor, including drugs or injury. Liver disease does not have any
effect, except at a very late stage when the patient is in hepatic failure. The
concentration of the blood alcohol does not influence the elimination rate. In
practice the rate will be constant regardless of whether the alcohol level is
0,10 or 0,20g%.
Pharmocodynamics in practice
We can assume that approximately 60% of an
ingested drink will be absorbed after 60 minutes and 90% after 90 minutes.
Alcohol elimination starts the moment the alcohol is distributed through the
body and reaches the liver. This happens at a constant rate.
As people seldom have only one drink, or gulp
down many drinks in a matter of minutes as if in one dose, it is obvious that
to plot a graph of someone's blood-alcohol level is not an easy task. Such a
graph is called the blood-alcohol curve (fig 11.2).
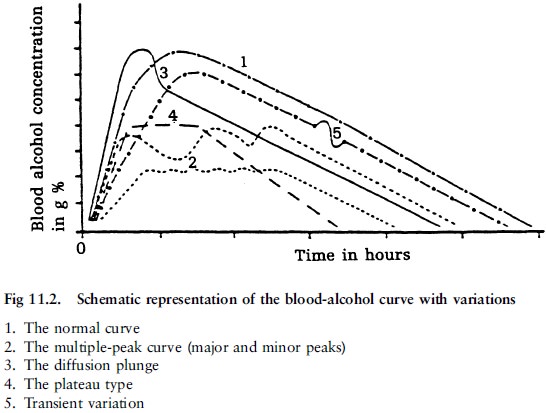
The ascending limb reflects that period when the
absorption rate is higher than the elimination rate. The gradient depends on
the rate of alcohol absorption, and the factors discussed above which may
affect it.
The peak will depend on the amount of alcohol
ingested. At this point the absorption rate equals the elimination rate. A
number of drinks over a longer period of time will result in multiple peaks. A
flatter curve with a plateau-like peak will result if alcohol is slowly
absorbed after a fatty meal for instance. The peak is usually reached after 15
to 90 minutes, but not later than 2 hours.
The limb going down reflects the period when the
elimination rate is higher than the absorption rate.
The Mellanby effect refers to the fact that a
person at a given blood-alcohol
level will present a different clinical picture,
depending on whether he/she is on the rising or declining limb of the curve.
The degree of intoxication will be more pronounced on the rising than the
declining limb because the brain will adapt to alcohol after a while due to the
development of acute alcohol tolerance.
Related Topics