Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Papovaviruses
Papilloma Virus :Clinical Aspects
PAPILLOMA VIRUS :CLINICAL ASPECTS
MANIFESTATIONS
Cutaneous warts can vary from flat to deep plantar growths. Although they can persist for years, they ultimately spontaneously regress. Respiratory papillomatosis due most often to types 6 and 11 occurs as intraoral or laryngeal lesions. These tend to occur in infants as a result of natal exposure, or in full grown adults.
External genital HPV infection occurs as exophytic genital warts (condyloma acumi-nata) caused most often by types 6 or 11. Lesions may increase in size to cauliflower-like appearance during pregnancy or immunosuppression. Genital HPV infection is most often benign, and many lesions reverse spontaneously. However they may become dysplastic and proceed through a continuum of cervical intraepithelial neoplasm to severe dysplasia and/or carcinoma in situ. The most common HPV in the malignant lesions is type 16, al-though this genotype, as well as the others, is most apt to cause lesions that regress sponta-neously. Higher grade malignancy is most apt to occur in the cervix, but the rate of anal carcinoma related to HPV appears to be increasing, especially in AIDS patients.
DIAGNOSIS
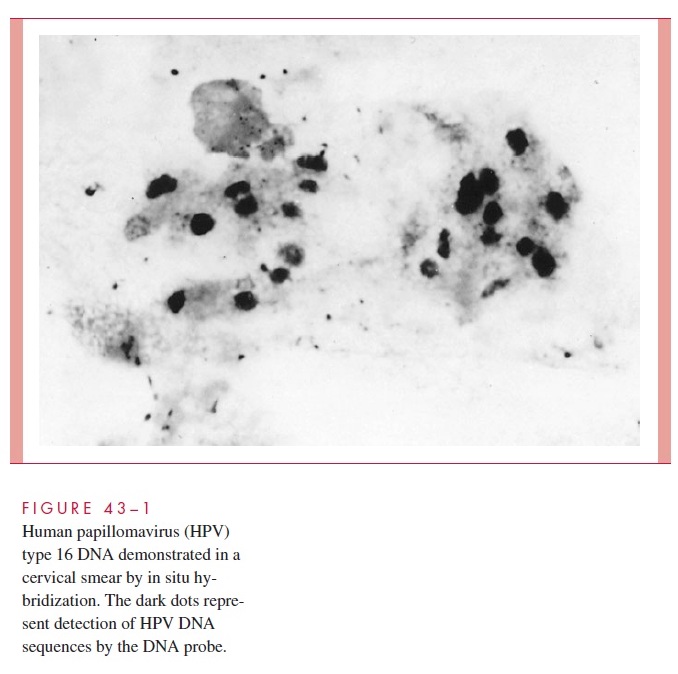
HPV does not grow in routine tissue culture, and antibody tests are rarely used. Papillo-mavirus infection leads to perinuclear cytoplasmic vacuolization and nuclear enlargement, referred to as poikilocytosis, in epithelial cells of the cervix or vagina. These changes can be seen in a routine Papanicolaou smear. The use of immunoassays to detect viral antigen and in situ hybridization or PCR to detect specific viral DNA in cervical swabs or tissue is more sensitive (Fig 43–1), but the clinical utility of detecting specific HPV types in clinical specimens remains to be determined. Detection of an abnormal cytology due to HPV should prompt colposcopy to assist in following or treating patients with abnormal lesions.
TREATMENT AND PREVENTION
Current treatment of HPV is usually either cytotoxic or surgical. Among the topical cytotoxins are podophyllin, podophyllotoxin, 5-fluorouracil, and trichloroacetic acid.
Recurrences are common following cessation of treatment because of survival of virus in the basal layers of the epithelium. Systemic and local interferon therapy has shown some promise as a treatment, although lesions tend to recur after cessation of therapy. Cervical lesions may be treated with electrocautery.
A recent large, prospective study of a HPV-16 virus-like-particle vaccine (an L1 polypeptide expressed in yeast) conducted among women 16 to 23 years of age indicated the potential for prevention of persistent infection, at least with this type, is high.
Related Topics