Chapter: Paediatrics: Neonatology
Paediatrics: Respiratory distress syndrome
Respiratory distress syndrome
RDS refers to lung disease caused
by surfactant deficiency. The disease is largely seen in preterm infants. RDS
is rare >32wks gestation.
Causes
Surfactant deficiency causes
alveolar collapse, increased work of breathing and hypoxia (due to
intrapulmonary shunting of blood). Increased risk of RDS is associated with CS
delivery; hypothermia; perinatal hypoxia; me-conium aspiration; congenital
pneumonia; maternal diabetes mellitus; past family history.
Presentation
Cyanosis, tachypnoea, chest in
drawing, grunting within 4hr of birth. If untreated, the disease worsens over
48ŌĆō72hr and then (depending on severity) resolves over 5ŌĆō7 days.
Investigations
ŌĆó
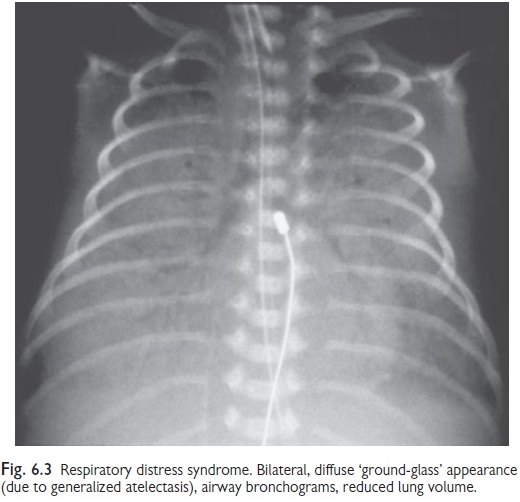
CXR: bilateral, diffuse ŌĆśground-glassŌĆÖ
appearance (generalized atelectasis),
airway bronchograms, reduced lung volume (see Fig, 6.3).
ŌĆó
SpO2
monitoring and blood gases.
Management
ŌĆó
Good
delivery room resuscitation. This may involve intubation and administration of
surfactant (extremely preterm) or nasal CPAP.
ŌĆó
Respiratory
support will depend on the severity. May need O2, nasal CPAP, or
ventilation.
ŌĆó
Surfactant
(Curosurf ® or Survanta®) requires intubation and
ventilation, and should be considered in all extremely preterm (<27/40)
infants and when oxygen requirement exceeds 30ŌĆō40%.
given as bolus down ETT;
give 2nd dose if oxygen
requirement remains high (FiO2>0.3);
ŌĆó
further
doses are sometimes required.
ŌĆó
Antibiotics: e.g. penicillin and gentamicin,
until congenital pneumonia has been
excluded, as it can mimic or coexist with RDS.
ŌĆó
Nutrition: use IV fluids until the baby is
stable. Then start gastric tube feeds
with minimal volumes and slowly increase as tolerated. If unstable, start
parenteral nutrition after 24ŌĆō48hr.
Prognosis
The majority have a good recovery.
Mortality is 5ŌĆō10% and depends on severity and gestation. Bronchopulmonary
dysplasia may develop (715% of cases, inversely proportional to gestational
age).
Prevention
ŌĆó
Corticosteroids
(betamethasone/dexamethasone, 2 doses, 12-hourly) given to mother 1ŌĆō7 days
before birth decreases incidence and mortality by 40%. Maximum benefit 24hr
after first dose and lasts 7 days.
ŌĆó
Treat
co-existing morbidities that inhibit surfactant production developing, e.g.
hypothermia, acidosis, infection.
Related Topics