Chapter: Paediatrics: Paediatric Surgery
Paediatrics: Congenital abnormalities: upper airway
Congenital abnormalities: upper airway
Choanal atresia (CA)
Congenital obstruction of the posterior
choana of the nose may be unilateral or bilateral. Babies are obligate nose
breathers and bilateral obstruction presents with asphyxia during feeding and
sleep. Unilateral obstruction may pass unnoticed. CA may be a presenting
feature of the CHARGE association, which is:
•
Coloboma;
•
Heart defects;
•
Atresia of the choanae;
•
Retardation of growth and
development;
•
Genitourinary abnormalities;
•
Ear abnormalities and hearing loss.
Diagnosis
•
NGT: the diagnosis is excluded by
passage of a tube down each nostril.
•
CT
scan will determine whether the obstruction is membranous or bony.
Treatment
•
Emergency
treatment comprises an oropharyngeal airway and an orogastric tube for feeding.
•
Surgery
(which is performed through a transnasal approach) restores the patency of the
choanae.
Laryngeal atresia
A rare condition that is
invariably fatal at birth. The condition is relatively easy to detect using
antenatal US because the foetal lungs appear bright and large. The large
airways can also be visualized because they are dis-tended with foetal lung
fluid. The condition is not amenable to correction (due to lung hypoplasia) and
termination of pregnancy should be offered.
Cleft lip and palate
Approximately 1 baby per 1000 is
born with a cleft lip and palate. This may occur sporadically or there may be a
family history. A cleft lip is immediately apparent. An isolated cleft palate
may not be noticed immediately, but will present with feeding difficulties,
particularly nasal regurgitation of milk. A cleft palate will interfere with
breastfeeding as it precludes generation of suction. Bottle-feeding may also be
difficult unless a squeezable bottle, rather than a rigid bottle, is used.
Management
•
Lip repair: at around 3mths of age.
•
Palate repair: at around 6mths of age.
Follow-up:
long-term because of problems with
speech, dentistry, and hearing.
Pierre–Robin sequence
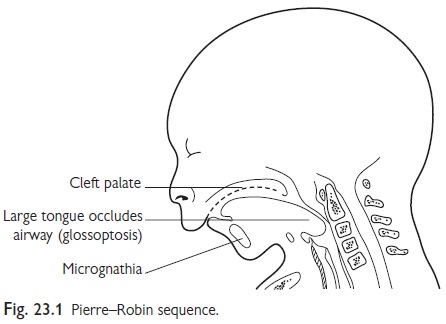
The Pierre–Robin sequence (Fig.
23.1) is characterized by three features:
•
micrognathia;
•
glossoptosis;
•
cleft
palate.
Management
•
The
large tongue has a tendency to obstruct the airway causing apnoea, particularly
during sleep.
•
Prone
positioning may help, allowing the tongue to fall forward, but occasionally
tracheostomy is necessary.
•
Endotracheal
intubation is often difficult.
•
Tube
feeding may be necessary.
•
The
palate is generally repaired between 9 and 18mths of age.
The airway problems invariably improve with growth.
Related Topics