Chapter: Paediatrics: Paediatric Surgery
Paediatrics: Anorectal malformations
Anorectal malformations
The incidence of anorectal
malformation is 1/5000 live births. Anorectal malformations comprise part of
the VACTERL association. The abnormality should be identified at birth. The
baby presents with:
ŌĆó
failure
to pass meconium;
ŌĆó
abdominal
distension;
ŌĆó
bile-stained
vomiting.
Anatomy
The precise anatomy varies but the
malformation can be subdivided into high and low/intermediate anomalies in
males and females.
Low/intermediate anomalies
ŌĆó
Rectum
is present and passes through a normal sphincter complex.
ŌĆó
In
boys (Fig. 23.17) there is a tiny fistulous track to the surface of the
perineum, often anteriorly on to the scrotum. If meconium is visible on the
perineum a local ŌĆścut-backŌĆÖ procedure can be performed to open the fistula back
to the rectum in anticipation of normal continence.
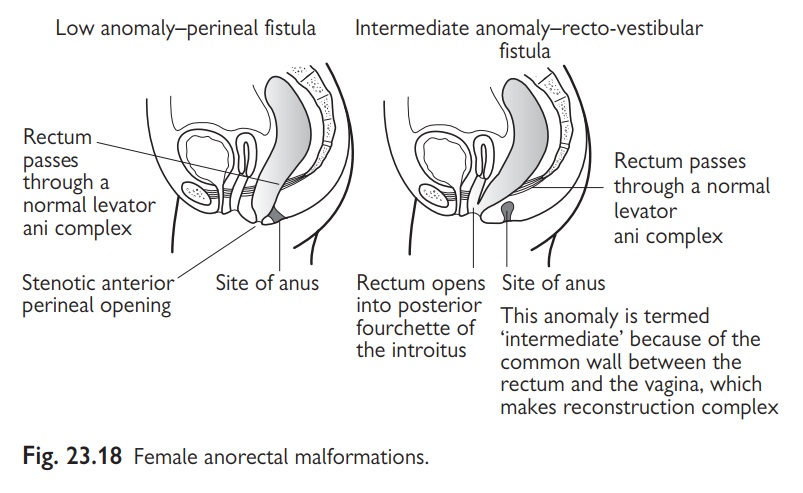
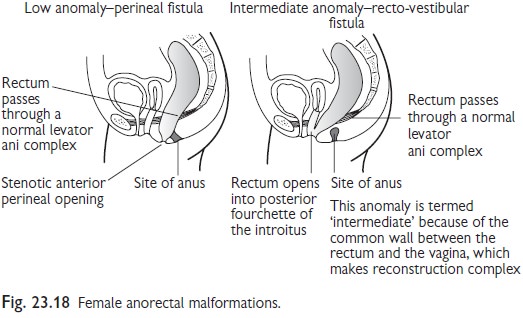
ŌĆó
In
girls (Fig. 23.18) the rectum usually opens into the back of the introitus as a
rectovestibular fistula. This abnormality is termed intermediate because,
although normal continence is to be expected, reconstruction involves division
of a common wall between rectum and vagina. For this reason treatment involves
a 3-stage procedure with defunctioning colostomy, anorectal reconstruction, and
then closure of the stoma.
ŌĆó
Vesicoureteric
reflux is very common.
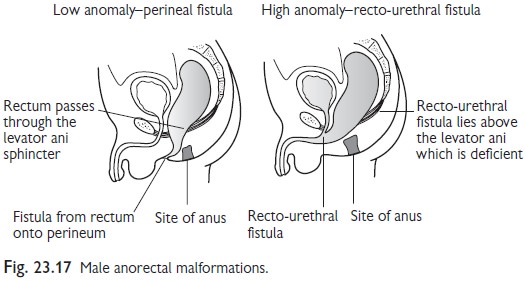
High anomalies
ŌĆó
These
anomalies are rare in girls but common in boys (Fig. 23.17).
ŌĆó
The
sphincter complex is poorly developed and the prospects for continence are
mediocre.
In boys the rectum makes a fistulous connection with the urethra. Treatment involves a defunctioning colostomy within the first 48hr of birth, reconstruction at a few months of age (most commonly involving a posterior sagittal anorectoplasty performed through a midline perineal incision), and then closure of the colostomy.
Related Topics