Chapter: Pathology: Respiratory Pathology
Obstructive Pulmonary Disease
OBSTRUCTIVE PULMONARY DISEASE
Chronic obstructive
pulmonary disease (COPD) is a general term used to
indicatechronic decreased respiratory function due to chronic bronchitis or
emphysema. Both diseases are associated with smoking.
Chronic
bronchitis
is a clinical diagnosis made when a patient has a persistent
coughand copious sputum production for at least 3 months in 2 consecutive
years. It is highly associated with smoking (90%). Clinical findings include
cough, sputum production, dyspnea, frequent infections, hypoxia, cyanosis, and
weight gain.
Microscopic
examination demonstrates hypertrophy and hyperplasia of bronchial mucous glands
(Reid index equals the submucosal gland thickness divided by the bronchial wall
thickness between the pseudostratified columnar epithelium and the
perichondrium; normal ratio is ≤0.4).
Complications
include increased risk for recurrent infections; secondary pulmonary
hypertension leading to right heart failure (cor pulmonale) and lung cancer.
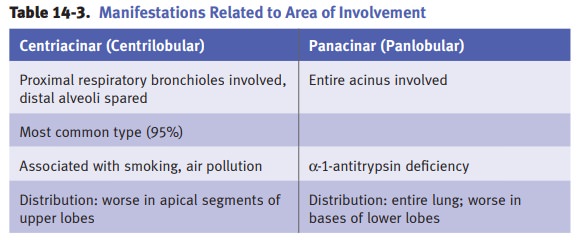
Emphysema
is the term used when destruction of alveolar septa results
in enlargedair spaces and a loss of elastic recoil. The 4 types of emphysema
are named for the anatomical distribution of the septal damage.
·
In centrilobular emphysema, the damage is in the proximal portion of
the acinus and the cause is cigarette smoking.
·
In panacinar emphysema, the damage affects the entire acinus and the
com-mon cause is alpha-1 antitrypsin deficiency.
·
In distal acinar emphysema (unknown cause), extension to the pleura
causes pneumothorax.
·
In irregular emphysema, post-inflammatory scarring involves the acinus
in an irregular distribution.
The
etiology of emphysema involves a protease/antiprotease
imbalance. On gross examination, the lungs are overinflated and enlarged,
and have enlarged, grossly visible air spaces. Clinical findings include
progressive dyspnea, pursing of lips and use of accessory respiratory muscles
to breathe, barrel chest (increased anterior-posterior diameter), and weight
loss.
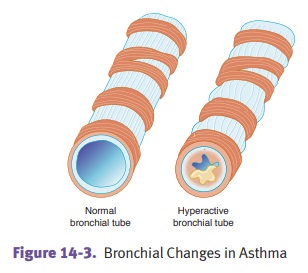
Asthma is
due to hyperreactive airways, which undergo episodic bronchospasmwhen triggered
by certain stimuli.
·
Atopic
(type I IgE-mediated hypersensitivity reaction) asthma (most
com-mon form) usually affects children and young adults. There is often a
positive family history.
·
Nonatopic
asthma is triggered by processes including respiratory
infections(usually viral), stress, exercise, or cold temperatures.
·
Drug-induced
asthma affects about 10% of adults with a diagnosis of
asthma.Aspirin is a key example of a precipitating drug.
·
Occupational
asthma is caused by workplace triggers including fumes anddusts.
An
asthma attack is characterized by wheezing, severe dyspnea, and coughing.
Prob-lems with expiration cause lung overinflation. Status asthmaticus is a
potentially fatal unrelenting attack of asthma.
Microscopic
examination of sputum cytology may show Curschmann spirals (twisted mucus plugs
admixed with sloughed epithelium), eosinophils, or Charcot-Leyden crystals
(protein crystalloids from broken down eosinophils).
In
patients dying from disease, autopsy findings include mucus plugs, increased
mucous glands with goblet cell hyperplasia, inflammation (especially with
eosino-phils), edema; hypertrophy and hyperplasia of bronchial wall smooth
muscle, and thickened basement membranes.
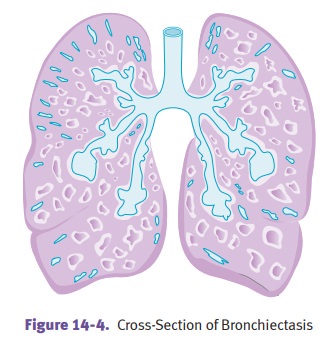
Bronchiectasis
is an abnormal permanent airway dilatation due to chronic
necro-tizing inflammation. Clinical findings include cough, fever, malodorous
purulent sputum, and dyspnea. Causes are diverse, and include bronchial
obstruction by for-eign body, mucus, or tumor, necrotizing pneumonias, cystic
fibrosis, and Kartagener syndrome.
·
Kartagener syndrome is an
autosomal recessive condition caused by immotilecilia due to a defect of dynein
arms (primary ciliary dyskinesia). It is character-ized clinically by
bronchiectasis, chronic sinusitis, and situs inversus (a con-genital condition
where the major visceral organs are anatomically reversed compared with their
normal anatomical positions).
On
gross examination, bronchiectasis shows dilated bronchi and bronchioles
extend-ing out to the pleura. These changes may also be appreciated on chest
x-ray. Compli-cations include abscess, septic emboli, cor pulmonale, and
secondary amyloidosis.
Related Topics