Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Biliary Disorders
Nursing Process: The Patient Undergoing Surgery for Gallbladder Disease
NURSING
PROCESS:THE PATIENT UNDERGOING SURGERY FOR GALLBLADDER DISEASE
Assessment
The
patient who is to undergo surgical treatment of gallbladder disease is often
admitted to the hospital or same-day surgery unit on the morning of surgery.
Preadmission testing is often com-pleted a week or more before admission; at
that time, the nurse instructs the patient about the need to avoid smoking to enhance
pulmonary recovery postoperatively and to avoid respiratory complications. It
also is important to instruct the patient to avoid the use of aspirin and other
agents (over-the-counter medications and herbal remedies) that can alter
coagulation and other bio-chemical processes.
Assessment
should focus on the patient’s respiratory status. If a traditional surgical
approach is planned, the high abdominal in-cision required during surgery may
interfere with full respiratory excursion. The nurse notes a history of
smoking, previous respi-ratory problems, shallow respirations, a persistent or
ineffective cough, and the presence of adventitious breath sounds. Nutri-tional
status is evaluated through a dietary history and general ex-amination
performed at the time of preadmission testing. The nurse also reviews
previously obtained laboratory results to ob-tain information about the
patient’s nutritional status.
Diagnosis
NURSING DIAGNOSES
Based
on all the assessment data, the major postoperative nursing diagnoses for the
patient undergoing surgery for gallbladder dis-ease may include the following:
•
Acute pain and discomfort related to surgical
incision
•
Impaired gas exchange related to the high abdominal
surgi-cal incision (if traditional surgical cholecystectomy is per-formed)
•
Impaired skin integrity related to altered biliary
drainage after surgical intervention (if a T-tube is inserted because of
retained stones in the common bile duct or another drainage device is employed)
•
Imbalanced nutrition, less than body requirements,
related to inadequate bile secretion
•
Deficient knowledge about self-care activities
related to in-cision care, dietary modifications (if needed), medications,
reportable signs or symptoms (eg, fever, bleeding, vomiting)
COLLABORATIVE PROBLEMS/ POTENTIAL COMPLICATIONS
Based
on assessment data, potential complications may include:
•
Bleeding
•
Gastrointestinal symptoms (may be related to
biliary leak)
Planning and Goals
The
goals for the patient include relief of pain, adequate ventila-tion, intact
skin and improved biliary drainage, optimal nutri-tional intake, absence of
complications, and understanding of self-care routines.
Postoperative Nursing Interventions
After
recovery from anesthesia, the nurse places the patient in the low Fowler’s
position. Intravenous fluids may be given, and na-sogastric suction (a
nasogastric tube was probably inserted im-mediately before surgery for a
nonlaparoscopic procedure) may be instituted to relieve abdominal distention.
Water and other fluids are given in about 24 hours, and a soft diet is started
when bowel sounds return.
RELIEVING PAIN
The
location of the subcostal incision in nonlaparoscopic gall-bladder surgery is
likely to cause the patient to avoid turning and moving, to splint the affected
site, and to take shallow breaths to prevent pain. Because full aeration of the
lungs and gradually in-creased activity are necessary to prevent postoperative
complications, the nurse should administer analgesic agents as prescribed to
relieve the pain and to promote well-being in addition to help-ing the patient
turn, cough, breathe deeply, and ambulate as in-dicated. Use of a pillow or
binder over the incision may reduce pain during these maneuvers.
IMPROVING RESPIRATORY STATUS
Patients
undergoing biliary tract surgery are especially prone to pulmonary
complications, as are all patients with upper abdom-inal incisions. Thus, the
nurse reminds patients to take deep breaths and cough every hour to expand the
lungs fully and prevent at-electasis. The early and consistent use of incentive
spirometry also helps improve respiratory function. Early ambulation prevents
pulmonary complications as well as other complications, such as
thrombophlebitis. Pulmonary complications are more likely to occur in the elderly
and in obese patients.
PROMOTING SKIN CARE AND BILIARY DRAINAGE
In
patients who have undergone a cholecystostomy or choledo-chostomy, the drainage
tubes must be connected immediately to a drainage receptacle. The nurse should
fasten tubing to the dress-ings or to the patient’s gown, with enough leeway
for the patient to move without dislodging or kinking it. Because a drainage
system remains attached when the patient is ambulating, the drainage bag may be
placed in a bathrobe pocket or fastened so that it is below the waist or common
duct level. If a Penrose drain is used, the nurse changes the dressings as
required.
After
these surgical procedures, the patient is observed for in-dications of
infection, leakage of bile into the peritoneal cavity, and obstruction of bile
drainage. If bile is not draining properly, an obstruction is probably causing
bile to be forced back into the liver and bloodstream. Because jaundice may
result, the nurse should be particularly observant of the color of the sclerae.
The nurse should also note and report right upper quadrant abdomi-nal pain,
nausea and vomiting, bile drainage around any drainage tube, clay-colored
stools, and a change in vital signs.
Bile
may continue to drain from the drainage tract in con-siderable quantities for a
time, necessitating frequent changes of the outer dressings and protection of
the skin from irritation be-cause bile is corrosive to the skin.
To prevent total loss of bile, the physician
may want the drainage tube or collection receptacle elevated above the level of
the abdomen so that the bile drains externally only if pressure develops in the
duct system. Every 24 hours, the nurse measures the bile col-lected and records
the amount, color, and character of the drainage. After several days of
drainage, the tube may be clamped for an hour before and after each meal to
deliver bile to the duodenum to aid in digestion. Within 7 to 14 days, the
drainage tube is removed. The patient who goes home with a drainage tube in
place requires instruction and reassurance about its function and care of the
tube.
In all
patients with biliary drainage, the nurse observes the stools daily and notes
their color. Specimens of both urine and stool may be sent to the laboratory
for examination for bile pig-ments. In this way, it is possible to determine
whether the bile pigment is disappearing from the blood and is draining again
into the duodenum. Maintaining a careful record of fluid intake and output is
important.
IMPROVING NUTRITIONAL STATUS
The
nurse encourages the patient to eat a diet low in fats and high in
carbohydrates and proteins immediately after surgery. At the time of hospital
discharge, there are usually no special dietary in-structions other than to
maintain a nutritious diet and avoid ex-cessive fats. Fat restriction usually
is lifted in 4 to 6 weeks when the biliary ducts dilate to accommodate the
volume of bile once held by the gallbladder and when the ampulla of Vater again
func-tions effectively. After this, when the patient eats fat, adequate bile
will be released into the digestive tract to emulsify the fats and allow their
digestion. This is in constrast to before surgery, when fats may not be
digested completely or adequately, and flatulence may occur. However, one
purpose of gallbladder surgery is to allow a normal diet.
MONITORING AND MANAGING POTENTIAL COMPLICATIONS
Bleeding
may occur as a result of inadvertent puncture or nick-ing of a major blood
vessel. Postoperatively, the nurse closely mon-itors vital signs and inspects
the surgical incisions and drains, if in place, for evidence of bleeding. The
nurse also periodically as-sesses the patient for increased tenderness and
rigidity of the ab-domen. If these signs and symptoms occur, they are reported
to the surgeon. The nurse instructs the patient and family to report to the
surgeon any change in the color of stools because this may indicate
complications. Gastrointestinal symptoms, although not common, may occur with
manipulation of the intestines during surgery.
After
laparoscopic cholecystectomy, the nurse assesses the pa-tient for loss of
appetite, vomiting, pain, distention of the ab-domen, and temperature
elevation. These may indicate infection or disruption of the gastrointestinal
tract and should be reported to the surgeon promptly. Because the patient is
discharged soon after laparoscopic surgery, the patient and family are
instructed verbally and in writing about the importance of reporting these
symptoms promptly.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-Care
The
nurse instructs the patient about the medications that are prescribed
(vitamins, anticholinergics, and antispasmodics) and their actions. It also is
important to inform the patient and fam-ily about symptoms that should be
reported to the physician, in-cluding jaundice, dark urine, pale-colored
stools, pruritus, or signs of inflammation and infection, such as pain or
fever.
Some
patients report one to three bowel movements a day. This is the result of a
continual trickle of bile through the chole-dochoduodenal junction after
cholecystectomy. Usually, such fre-quency diminishes over a period of a few
weeks to several months.
If a
patient is discharged from the hospital with a drainage tube still in place,
the patient and family may need instructions about its management. The nurse
instructs them in proper care of the drainage tube and the importance of
reporting to the physician promptly any changes in the amount or
characteristics of drainage. Assistance in securing the appropriate dressings will
reduce the patient’s anxiety about going home with the drain or tube still in
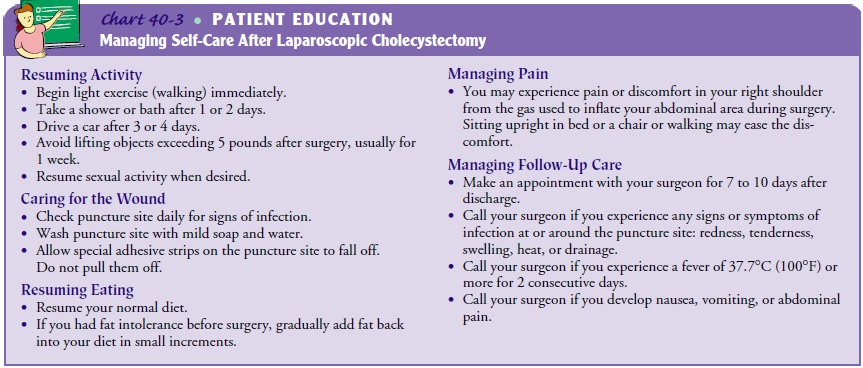
place. (See Chart 40-3 for more details.)
Continuing Care
With sufficient support at home, most patients recover quickly from cholecystectomy. However, elderly or frail patients and those who live alone may require a referral for home care. During home visits, the nurse assesses the patient’s physical status, especially wound healing, and progress toward recovery. Assessing the patient for adequacy of pain relief and pulmonary exercises also is impor-tant. If the patient has a drainage system in place, the nurse assesses it for patency and appropriate management by the patient and fam-ily.
Assessing for signs of infection and teaching the patient about the
signs and symptoms of infection are also important nursing in-terventions. The
patient’s understanding of the therapeutic regimen (medications, gradual return
to normal activities) is assessed, and previous teaching is reinforced. The
nurse emphasizes the impor-tance of keeping follow-up appointments and reminds
the patient and family of the importance of participating in health promotion
activities and recommended health screening.
Evaluation
EXPECTED PATIENT OUTCOMES
Expected
patient outcomes may include:
•
Reports decrease in pain
a)
Splints abdominal incision to decrease pain
b)
Avoids foods that cause pain
c)
Uses postoperative analgesia as prescribed
•
Demonstrates appropriate respiratory function
a) Achieves full
respiratory excursion, with deep inspira-tion and expiration
b) Coughs effectively,
using pillow to splint abdominal incision
c)
Uses postoperative analgesia as prescribed
d)
Exercises as prescribed (eg, turns, ambulates)
•
Exhibits normal skin integrity around biliary
drainage site (if applicable)
a)
Is free of fever, abdominal pain, change in vital
signs, or bile, foul-smelling drainage, or pus around drainage tube
b)
Demonstrates proper management of drainage tube (if
applicable)
c)
Identifies signs and symptoms of biliary
obstruction to be noted and reported
d)
Has serum bilirubin level within normal range
•
Obtains relief of dietary intolerance
a) Maintains adequate
dietary intake and avoids foods that cause gastrointestinal symptoms
b)
Reports decreased or absent nausea, vomiting,
diarrhea, flatulence, and abdominal discomfort
•
Absence of complications
a)
Has normal vital signs (blood pressure, pulse,
respira-tory rate and pattern, and temperature)
b)
Reports absence of bleeding from gastrointestinal
tract, biliary drainage tube/catheter (if present) and no evi-dence of bleeding
in stool
c)
Reports return of appetite and no evidence of
vomiting, abdominal distention, and pain
d)
Lists symptoms that should be reported to surgeon
promptly and demonstrates an understanding of self-care, including wound care
Related Topics