Chapter: Medical Physiology: Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Normal Heart Sounds
Heart Sounds
Normal Heart Sounds
Listening with a stethoscope to a normal heart, one hears a sound usually described as “lub, dub, lub, dub. ”The “lub” is associated with closure of the atrio-ventricular (A-V) valves at the beginning of systole, and the “dub” is associated with closure of the semilunar (aortic and pulmonary) valves at the end of systole. The “lub” sound is called the first heart sound, and the “dub” is called the second heart sound, because the normal pumping cycle of the heart is con-sidered to start when the A-V valves close at the onset of ventricular systole.
Causes of the First and Second Heart Sounds. The earliest explanation for the causeof the heart sounds was that the “slapping” together of the valve leaflets sets up vibrations. However, this has been shown to cause little, if any, of the sound, because the blood between the leaflets cushions the slapping effect and pre-vents significant sound. Instead, the cause is vibration of the taut valves imme-diately after closure, along with vibration of the adjacent walls of the heart and major vessels around the heart. That is, in generating the first heart sound, con-traction of the ventricles first causes sudden backflow of blood against the A-V valves (the tricuspid and mitral valves), causing them to close and bulge toward the atria until the chordae tendineae abruptly stop the back bulging. The elastic tautness of the chordae tendineae and of the valves then causes the back surging blood to bounce forward again into each respective ventricle. This causes the blood and the ventricular walls, as well as the taut valves, to vibrate and causes vibrating turbulence in the blood. The vibrations travel through the adjacent tissues to the chest wall, where they can be heard as sound by using the stethoscope.
The second heart sound results from sudden closure of the semilunar valves at the end of systole. When the semilunar valves close, they bulge backward toward the ventricles, and their elastic stretch recoils the blood back into the arteries, which causes a short period of reverberation of blood back and forth between the walls of the arteries and the semilunar valves, as well as between these valves and the ventricular walls. The vibrations occurring in the arterial walls are then transmitted mainly along the arteries. When the vibrations of the vessels or ventricles come into contact with a “sounding board,” such as the chest wall, they create sound that can be heard.
Duration and Pitch of the First and Second Heart Sounds. Theduration of each of the heart sounds is slightly more than 0.10 second—the first sound about 0.14 second, and the second about 0.11 second. The reason for the shorter second sound is that the semilunar valves are more taut than the A-V valves, so that they vibrate for a shorter time than do the A-V valves.
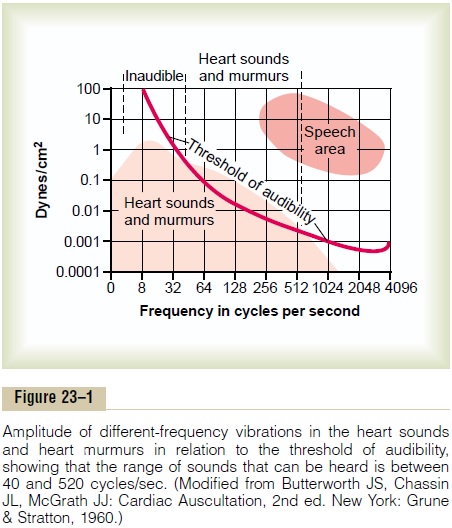
The audible range of frequency (pitch) in the first and second heart sounds, as shown in Figure 23–1, begins at the lowest frequency the ear can detect, about 40 cycles/sec, and goes up above 500 cycles/sec. When special electronic apparatus is used to record these sounds, by far a larger proportion of the re-corded sound is at frequencies and sound levels below the audible range, going down to 3 to 4 cycles/sec and peaking at about 20 cycles/sec, as illustrated by the lower shaded area in Figure 23–1. For this reason, major portions of the heart sounds can be recorded electronically in phonocardiograms even though they cannot be heard with a stethoscope.
The second heart sound normally has a higher fre-quency than the first heart sound for two reasons: (1) the tautness of the semilunar valves in comparison with the much less taut A-V valves, and (2) the greater elastic coefficient of the taut arterial walls that provide the principal vibrating chambers for the second sound, in comparison with the much looser, less elastic ven-tricular chambers that provide the vibrating system for the first heart sound. The clinician uses these differ-ences to distinguish special characteristics of the two respective sounds.
Third Heart Sound. Occasionally a weak, rumbling thirdheart sound is heard at the beginning of the middle this sound is oscillation of blood back and forth between the walls of the ventricles initiated by inrush-ing blood from the atria. This is analogous to running water from a faucet into a paper sack, the inrushing water reverberating back and forth between the walls of the sack to cause vibrations in its walls. The reason the third heart sound does not occur until the middle third of diastole is believed to be that in the early part of diastole, the ventricles are not filled sufficiently to create even the small amount of elastic tension neces-sary for reverberation. The frequency of this sound is usually so low that the ear cannot hear it, yet it can often be recorded in the phonocardiogram.
Atrial Heart Sound (Fourth Heart Sound). An atrial heartsound can sometimes be recorded in the phonocar-diogram, but it can almost never be heard with a stethoscope because of its weakness and very low frequency—usually 20 cycles/sec or less. This sound occurs when the atria contract, and presumably, it is caused by the inrush of blood into the ventricles, which initiates vibrations similar to those of the third heart sound.
Chest Surface Areas for Auscultation of Normal Heart Sounds
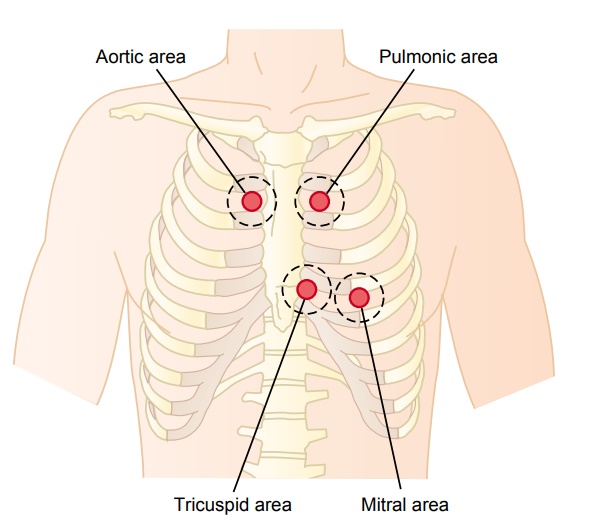
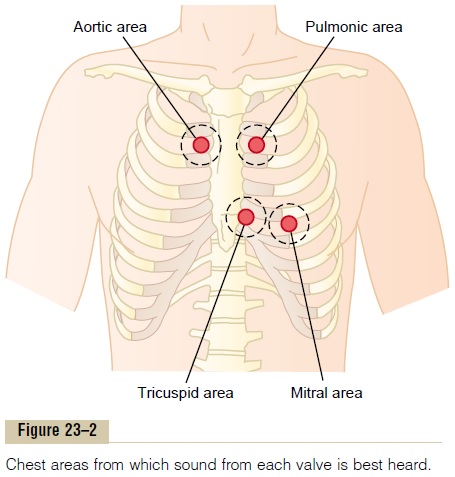
Listening to the sounds of the body, usually with the aid of a stethoscope, is called auscultation. Figure 23–2 shows the areas of the chest wall from which the dif-ferent heart valvular sounds can best be distinguished. Although the sounds from all the valves can be heard from all these areas, the cardiologist distinguishes the sounds from the different valves by a process of
elimination. That is, he or she moves the stethoscope from one area to another, noting the loudness of the sounds in different areas and gradually picking out the sound components from each valve.
The areas for listening to the different heart sounds are not directly over the valves themselves. The aortic area is upward along the aorta because of sound trans-mission up the aorta, and the pulmonic area is upward along the pulmonary artery. The tricuspid area is over the right ventricle, and the mitral area is over the apex of the left ventricle, which is the portion of the heart nearest the surface of the chest; the heart is rotated so that the remainder of the left ventricle lies more posteriorly.
Phonocardiogram
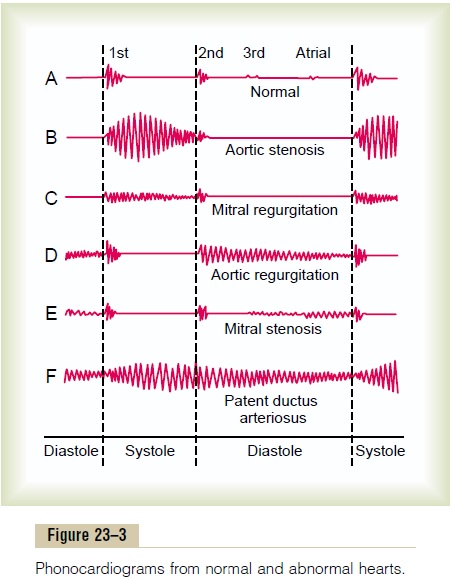
If a microphone specially designed to detect low-fre-quency sound is placed on the chest, the heart sounds can be amplified and recorded by a high-speed record-ing apparatus. The recording is called a phonocardio-gram, and the heart sounds appear as waves, as shownschematically in Figure 23–3. Recording A is an example of normal heart sounds, showing the vibra-tions of the first, second, and third heart sounds and even the very weak atrial sound. Note specifically that the third and atrial heart sounds are each a very low rumble. The third heart sound can be recorded in only one third to one half of all people, and the atrial heart sound can be recorded in perhaps one fourth of all people.
Related Topics