Chapter: Surgical Pathology Dissection : The Digestive System
Local or Segmental Biliary Resections: Surgical Pathology Dissection
Local or Segmental Biliary Resections
The
extrahepatic bile ducts are most commonly encountered as part of a
pancreaticoduodenec-tomy (including the distal common bile duct) and partial or
total hepatectomy (including portions of the proximal extrahepatic biliary
tree). Exami-nation of the bile ducts in these specimens is described elsewhere
in this book. Local or seg-mental resections of the extrahepatic bile ducts are
less common but may be performed for carci-noma of the extrahepatic bile ducts,
isolated stric-tures, or choledochal cysts.
The
specimen should first be oriented, prefera-bly as indicated by the surgeon or
by noting its relationship to the gallbladder. Note if the spec-imen is
received fixed or unfixed, whether it has been previously incised, and whether
other tissues or organs accompany the bile duct. Mea-sure the length and
diameter of each portion of the biliary tree that is present. Describe the
ap-pearance of the external surface, including the presence of any mass lesions
or adhesions. In general, the proximal and distal bile duct margins and the
periductal soft tissue (forming the circumferential margin of the excision)
should then be inked because of the high likelihood of carcinoma.
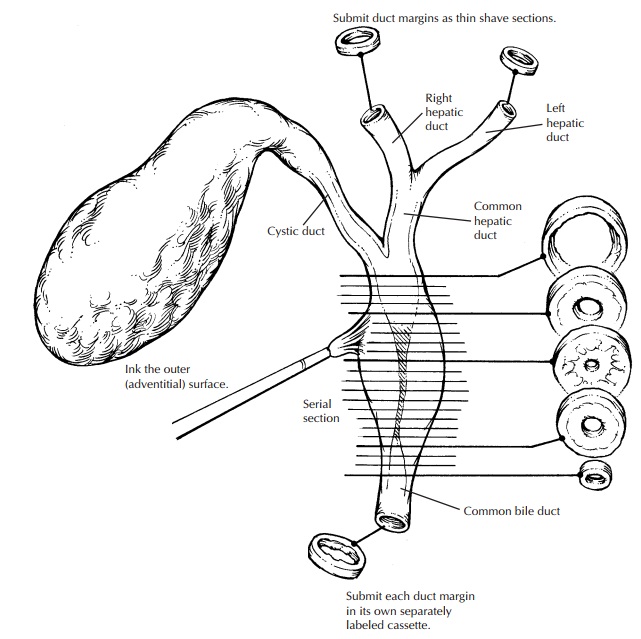
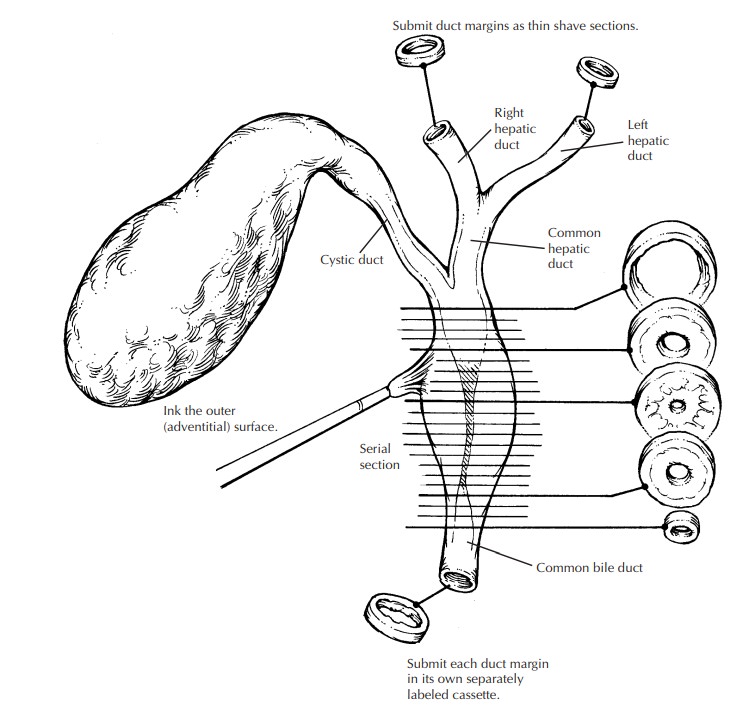
It is
best not to attempt to open the ducts lon-gitudinally, since small papillary
lesions in the ducts could easily be dislodged and the mucosa disrupted by the
scissors. Instead, make serial cross sections at 2- to 3-mm intervals with a
scalpel, keeping the cross sections oriented with regard to the segment of the
biliary tree and the proximal and distal margins. The resulting cross sections
can then be examined for the presence of any obstructing lesions in the lumen,
the presence of a mass, or the presence of a stricture. If a stric-ture is
present, describe its location and measure its length, the sizes of the bile
duct lumen at, above, and below the stricture, and the thickness of the bile
duct wall in the region of the stricture and elsewhere. Carcinoma of the bile
ducts can infiltrate diffusely into the bile duct wall and thereby mimic a
benign stricture, or it can have a papillary or nodular configuration. If a
calculus, papillary lesion, or mass is seen, describe its loca-tion, whether it
obstructs the lumen, and whether there is obvious penetration of the bile duct
wall and involvement of any adjacent structures. In general, the specimen should
then be submitted in its entirety in serial cross sections, keeping the
proximal and distal shave margins separate. (Surgically resectable carcinomas
of the bile ducts are unlikely to be too large to submit in toto, and segmental
bile duct resections without a grossly obvious tumor would have to be
completely em-bedded anyway.)
Choledochal
cysts should also be inked along the external surface. Measure the dimensions
of the cyst and describe its configuration (e.g., fusi-form or saccular).
Carefully incise the cyst with a scalpel and drain the contents into a
container. Note the volume and type of the fluid present (bile, blood, fibrin,
mucoid material, pus). After draining the cyst contents, open the cyst
longitu-dinally with a small pair of scissors and examine the inner lining.
Specifically, describe the appear-ance of the lining (often denuded,
bile-stained, and shaggy) and the presence of any visible islands of residual
mucosa. Are any masses or suspicious lesions present? The risk of carcinoma
developing within choledochal cysts increases with age, and up to 15% of
choledochal cysts in adults harbor a carcinoma. If a suspicious lesion is
present, describe its dimensions, color, con-sistency, associated necrosis, and
how deeply it penetrates the cyst wall.
Representative
full-thickness sections of the cyst should be taken. They should include
ap-proximately one section per centimeter of cyst wall diameter as well as
proximal and distal shave margins. If any suspicious lesions are pres-ent,
additional sections are needed, including full-thickness sections of the lesion
at its deepest extent and sections that demonstrate the interface between the
lesion and the adjacent cyst wall.
Related Topics