Chapter: Microbiology and Immunology: Virology, Virus: Paramyxoviruses
Laboratory Diagnosis - Measles Virus Infections
Laboratory Diagnosis
The clinical manifestations of typical measles cases are so char-acteristic that the diagnosis is self-evident. The laboratory diag-nosis is frequently helpful to diagnose atypical measles and to differentiate from rubella.
◗ Specimens
Respiratory specimens, conjunctival specimens, urine, blood, and brain tissues are the frequently used specimens. The respiratory specimens and blood collected during the prodromal stage and the period following until 2 days after the appearance of the rash are the specimens of choice for isolation of viruses by culture.
◗ Microscopy
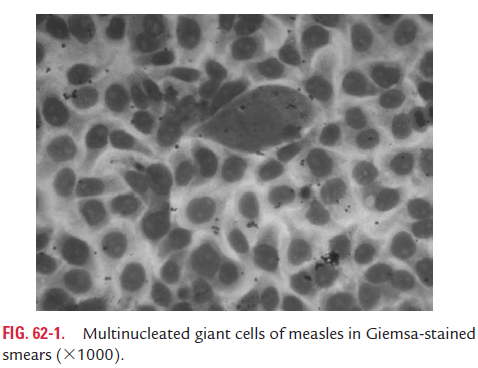
Demonstration of multinucleated giant cells, measuring up to 100 nm in diameter, in Giemsa-stained smears is diagnos-tic of measles (Fig. 62-1, Color Photo 58). These giant cells can be demonstrated in biopsies of Koplik’s spots, nasal secretion smears, and in dermal rashes.
◗ Direct antigen detection
Measles antigen can be detected in nasal secretions, pharyngeal secretions, or in urinary sediments by direct immunofluores-cence antibody test.
◗ Isolation of the virus
The measles virus is difficult to isolate, but it can be grown in primary human or monkey kidney cell cultures. The virus pro-duces cytopathic effects (CPEs) very slowly, usually 1 week after inoculation. The viral antigen appearing in the infected cell cultures, however, can be detected much earlier by using direct immunofluorescence antibody test.
◗ Serodiagnosis
Sandwich capture IgM enzyme-linked immunosorbent assay (IgM ELISA) is the quickest method to diagnose acute measles by detection of IgM antibodies in the serum. The IgM antibod-ies begin to appear in the serum on the third day after appear-ance of rash and remain positive 30–60 days after illness in most individuals suffering from measles. The test is therefore positive during these days. IgM ELISA is highly sensitive (nearly 100%) during this period of illness. The IgM antibody is usually not positive in the first 2 days after appearance of rash; in some individuals, IgM antibodies may become negative 30 days after the onset of rash.
Demonstration of more than fourfold rise in IgG antibody titer between acute and convalescent sera confirms diagnosis of measles. IgG antibodies usually appear 4 days after the onset of rash and persist for a longer period even after the patient has been cured of the illness. Demonstration of unusually high titer of measles antibody in the serum and CSF is diagnostic of SSPE.
Treatment
Ribavirin given either intravenous or in aerosol form is being now evaluated to treat severely affected adults and immuno-compromised individuals with acute measles or SSPE. Measles virus has been shown to be susceptible to ribavirin in vitro. However, the drug is yet to be used for regular treatment of cases of measles, since no controlled trials have been conducted to test the efficacy of the drug in patients with measles.
Related Topics