Chapter: Obstetrics and Gynecology: Abnormal Labor and Intrapartum Fetal Surveillance
Intrapartum Fetal Surveillance: Pathophysiology
Pathophysiology
The uteroplacental unit provides oxygen and nutrients to the fetus
while receiving carbon dioxide and wastes, the products of the normal aerobic
fetal metabolism. Uteroplacental
insufficiency occurs when the utero-placental unit is compromised. Initial
fetal responses include fetal hypoxia (decreased blood oxygen levels); shunting
of blood flow to the fetal brain, heart, and adrenal glands; and transient,
repetitive, late decelerations of the FHR. If hypoxia continues, the fetus will
eventually switch over to anaerobic glycolysis and develop meta-bolic acidosis.
Lactic acid accumulates and progressive damage to vital organs occurs,
especially the fetal brain and myocardium. If intervention is not timely,
serious and possibly permanent damage and sometimes death can result.
Neonatal
encephalopathy is a clinically defined syn-drome of disturbed
neurologic function in the earliest days of life in the term infant, manifested
by difficulty with initiating and maintaining respiration, depression of tone
and reflexes, subnormal level of consciousness, and some-times seizures.
Neonatal encephalopathy is not always as-sociated with permanent neonatal
neurologic impairment. Hypoxic-ischemic
encephalopathy (HIE) is a subtypeof neonatal encephalopathy for which the cause
is consid-ered to be limitation of oxygen and blood flow near the time of
birth. Historically, it has been assumed that most cases of neonatal
encephalopathy were hypoxic-ischemic encephalopathy, but epidemiologic studies
have estab-lished that this assumption is incorrect.
Approximately
70% of cases of neonatal encephalopathy are caused by factors that were present
before the onset of labor.
It is estimated that the
incidence of neonatal encephalop-athy caused by intrapartum hypoxia is
approximately 1.6/10,000, absent other coincident preconceptual or an-tepartum
abnormalities. HIE is thus one item in the larger category of encephalopathies
which may result from con-ditions such as prenatal stroke, prenatal infection,
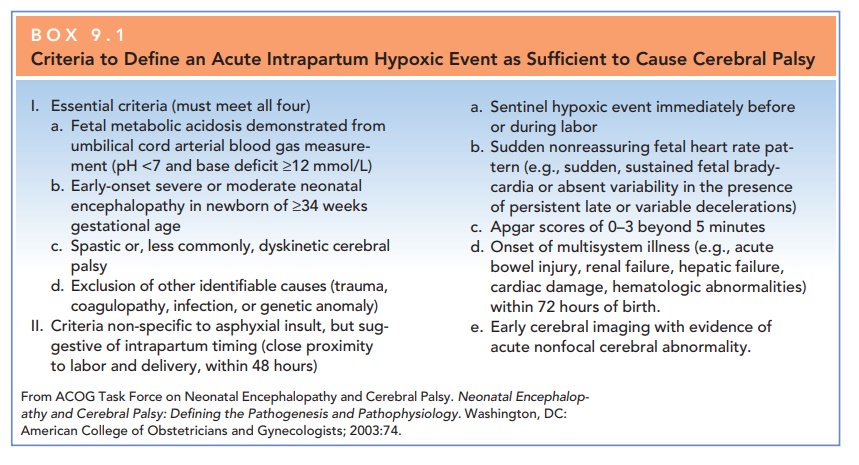
genetic abnormalities, and neonatal cerebral malformation. The criteria
sufficient to suggest that an encephalopathy is as-sociated with an acute
intrapartum event are presented in Box 9.1.
Cerebral
palsy is a chronic disability of the centralnervous
system (CNS) characterized by aberrant control of movement and posture
appearing early in life and not as a result of progressive neurologic disease.
Only one type of cerebral palsy, spastic
quadriplegia, is associated with antepartum or intrapartum interruption of
the fetal blood supply. Disorders not associated with intrapartum or peripartum
asphyxia include dyskinetic or ataxic cere-bral palsy (which commonly has a
genetic origin) and epilepsy, mental retardation, or attention-deficit
hyper-activity disorders.
Related Topics