Chapter: Medicine and surgery: Endocrine system
Hyperprolactinaemia - Dopamine and prolactin axis
Hyperprolactinaemia
Definition
Hyperprolactinaemia is a raised serum prolactin level causing galactorrhoea and gondadal dysfunction.
Incidence
Most common endocrine abnormality of the hypothalamic–pituitary axis.
Aetiology
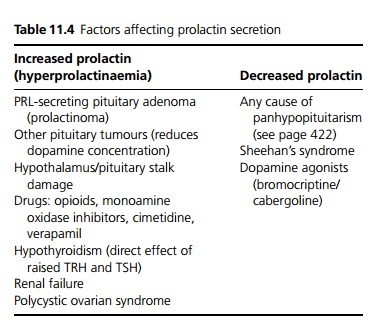
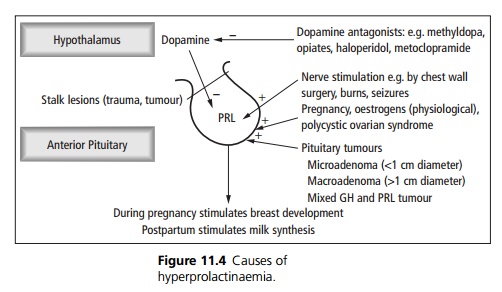
Prolactin (PRL) is under the inhibitory control of dopamine released from the hypothalamus. Causes of hyperprolactinaemia are shown in Fig. 11.4 and Table 11.4.
Pathophysiology
Hyperprolactinaemia causes disturbance of the hypothalamic–pituitary–gonadal axis in both men and women, probably by a local hormonal interaction between prolactin and hypothalamic gonadotrophinreleasing hormone (GnRH) secretion.
· Gonadotrophin (luteinising hormone and follicle stimulating hormone (LH and FSH) secretion is abnormal and the midcycle surge in LH in women is suppressed.
· Hyperprolactinaemia in women is commonly physiological, and in men it is almost always of pathological significance.
Clinical features
In women hyperprolactinaemia causes primary or secondary amenorrhoea, oligomenorrhoea with anovulation or infertility. Galactorrhoea is variably present. Oestrogen deficiency can cause vaginal dryness and osteopenia. Hirsutism can occur, with weight gain and anxiety depression and hot flushes. In men galactorrhoea occurs occasionally, but the most common early features are decreased libido and sexual dysfunction, sometimes with impotence and infertility.
Complications
Headache, visual impairment and hypopituitarism due to local effects of the adenoma.
Investigations
Raised PRL in the absence of another cause of hyper-prolactinaemia is the feature of a functioning pituitary adenoma. The serum prolactin level is in proportion to tumour size. All the pituitary hormone axes have to be tested to look for associated hypopituitarism. Plain skull X-ray is usually normal, whereas MRI will demonstrate the lesion, usually <1 cm in size.
Management
Prolactinomas are treated with dopaminergic drugs such as cabergoline. The minority of tumours that do not respond to medical treatment and hyperprolactinaemia due to stalk compression are treated surgically.
Related Topics