Chapter: Clinical Dermatology: Regional dermatology
Hirsutism and hypertrichosis
Hirsutism
and hypertrichosis
Hirsutism
is the growth of terminal hair in a female (Fig. 13.15), which is distributed
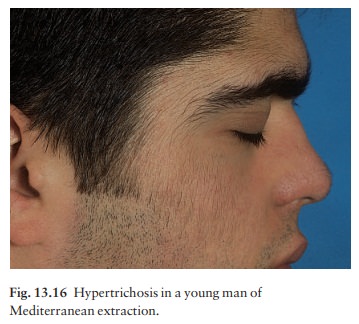
in the pattern norm-ally seen in a male. Hypertrichosis is an excessive growth
of terminal hair that does not follow an androgen-induced pattern (Fig. 13.16)

Cause
Some
degree of hirsutism may be a racial or familial trait, and minor facial
hirsutism is common after the menopause. In addition, some patients without a
family background of hirsutism become hirsute in the absence of any
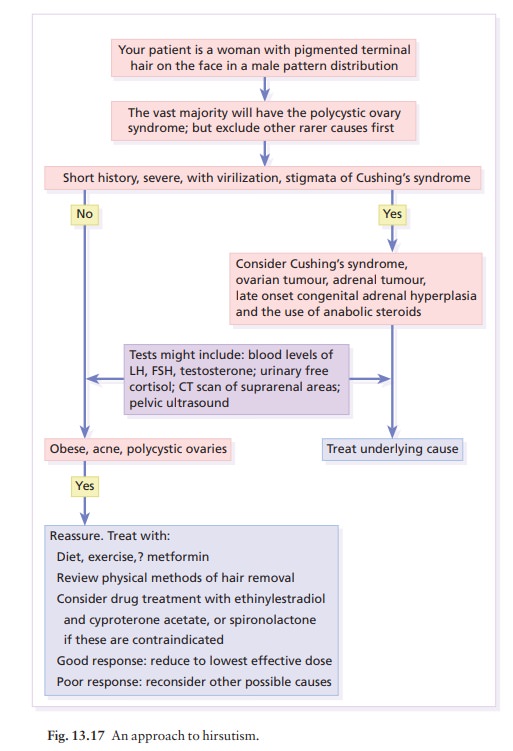
demonstrable hormonal cause (idiopathic hirsutism). Finally, some patients with
hirsutism will have one of the disorders shown in Fig. 13.17.
Presentation
An
excessive growth of hair appears in the beard area, on the chest and
shoulder-tips, around the nipples and in the male pattern of pubic hair.
Androgenetic alopecia may complete the picture.
Course
Familial,
racial or idiopathic hirsutism tends to start at puberty and to worsen with
age.
Complications
Virilization
causes infertility; psychological disturb-ances are common.
Investigations
Significant
hormonal abnormalities are not usually found in patients with a normal
menstrual cycle.
Investigations
are needed:
•
if hirsutism occurs in childhood;
•
if there are other features of
virilization, such as clitoromegaly;
•
if the hirsutism is of sudden or
recent onset; or
• if there is menstrual irregularity or cessation.
The
tests used will include measurement of the serum testosterone,
sex-hormone-binding globulin, dehy-droepiandrosterone sulphate, androstenedione
and prolactin. Ovarian ultrasound is useful if polycystic ovaries are
suspected.
Treatment (Fig. 13.17)
Any underlying disorder must be treated on its merits. Home remedies for minor hirsutism include commercial
depilatory creams (often containing a thioglycollate), waxing or shaving, or
making the appearance less obvious by bleaching; none remove the hair
per-mamently. Plucking should probably be avoided as it can stimulate hair
roots into anagen. The abnormally active follicles, if relatively few, can be
destroyed by electrolysis. If the hairs are too numerous for this, the excess
can be removed by laser. Topical therapy with eflornithine, an inhibitor of
ornithine decarboxylase, can slow regrowth. Oral antiandrogens (e.g.
cyproterone acetate; Dianette) may sometimes be helpful, but will be needed
long-term. Pregnancy must be avoided during such
treatment
as it carries the risk of feminizing a male fetus. Spironolactone is used less
often now.
Related Topics