Chapter: Clinical Dermatology: Infections
Herpangina, Measles, Rubella, Erythema infectiosum
Herpangina
This is an acute infectious illness, caused by group A Coxsackie viruses. The patient is usually a child with a fever, and a severe sore throat covered in many small vesicles, which rapidly become superficial ulcers. Episodes resolve in about a week.
Hand, foot and mouth disease
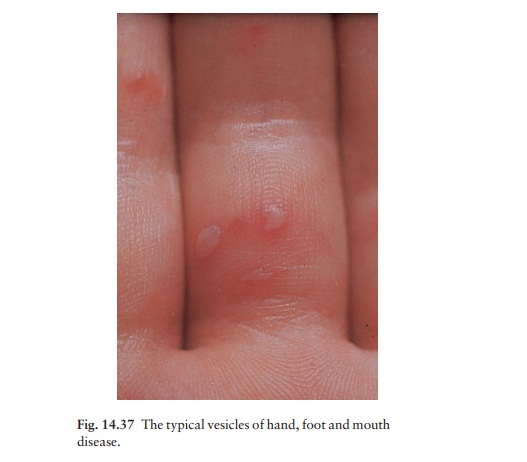
This
is usually caused by Coxsackie A16. Minor epidemics occur in institutions. The
oral vesicles are larger and fewer than those of herpangina. The hand and foot
lesions are small greyish vesicles with a narrow rim of redness around (Fig.
14.37). The con-dition settles within a few days.

Measles
An
incubation period of 10 days is followed by fever, conjunctival injection,
photophobia and upper respira-tory tract catarrh. KoplikŌĆÖs spots (pinhead sized
white spots with a bright red margin) are seen at this stage on the buccal
mucosa. The characteristic ŌĆśnet-likeŌĆÖ rash starts after a few days, on the brow
and behind the ears, and soon becomes extensive before fading with much
desquamation. Prevention is by immunization with the combined MMR
(measles/mumps/rubella) vaccine.
Rubella
After an incubation period of about 18 days, lym-phadenopathy occurs a few days before the evanescent pink macular rash, which fades, first on the trunk, over the course of a few days. Rubella during the first trimester of pregnancy carries a risk of damage to the unborn child. Prevention is by immunization with the combined MMR vaccine.
Erythema infectiosum (fifth disease)
This
is caused by the human parvovirus B19 and occurs in outbreaks, often in the
spring. A slapped cheek erythema is quickly followed by a reticulate erythema
of the shoulders. The affected child feels well, and the rash clears over the
course of a few days. Other features, sometimes not accompanied by a rash,
include transient anaemia and arthritis.
Related Topics