Chapter: Medical Surgical Nursing: Assessment of Respiratory Function
Health History - Assessment of Respiratory Function
Assessment
HEALTH HISTORY
The health history focuses on the physical
and functional prob-lems of the patient and the effect of these problems on his
or her life. The reason the patient is seeking health care often is related to
one of the following: dyspnea
(shortness of breath), pain, ac-cumulation of mucus, wheezing, hemoptysis (blood spit up from the
respiratory tract), edema of the ankles and feet, cough, and general fatigue
and weakness.
In
addition to identifying the chief reason why the patient is seeking health
care, the nurse tries to determine when the health problem or symptom started,
how long it lasted, if it was relieved at any time, and how relief was
obtained. The nurse collects in-formation about precipitating factors,
duration, severity, and as-sociated factors or symptoms and also assesses for
risk factors and genetic factors that may contribute to the patient’s lung
condi-tion (Chart 21-5).
The nurse assesses the impact of signs
and symptoms on the patient’s ability to perform activities of daily living and
to partic-ipate in usual work and family activities. In addition, psychoso-cial
factors that may affect the patient are explored (Chart 21-6). These factors
include anxiety, role changes, family relationships, financial problems,
employment status, and the strategies the pa-tient uses to cope with them.
Many
respiratory diseases are chronic and progressively debil-itating. Therefore,
ongoing assessment of the patient’s physical abilities, psychosocial supports,
and quality of life is needed to plan appropriate interventions. It is
important for the patient with a respiratory disorder to understand the
condition and to be familiar with necessary self-care interventions. The nurse
evalu-ates these factors over time and provides education as needed.
Signs and Symptoms
The
major signs and symptoms of respiratory disease are dyspnea, cough, sputum
production, chest pain, wheezing, clubbing of the fingers, hemoptysis, and
cyanosis. These clinical manifestations are related to the duration and
severity of the disease.
DYSPNEA
Dyspnea (difficult or labored breathing, shortness of breath) is a symptom common to many pulmonary and cardiac disorders, particularly when there is decreased lung compliance or increased airway resistance. The right ventricle of the heart will be affected ultimately by lung disease because it must pump blood through the lungs against greater resistance. It may also be associated with neurologic or neuromuscular disorders such as myasthenia gravis, Guillain-Barré syndrome, or muscular dystrophy.
Clinical Significance.
In general, acute diseases of the lungs
pro-duce a more severe grade of dyspnea than do chronic diseases. Sudden
dyspnea in a healthy person may indicate pneumothorax (air in the pleural
cavity), acute respiratory obstruction, or ARDS. In immobilized patients,
sudden dyspnea may denote pulmonary embolism. Orthopnea (inability to breathe easily except in an upright
position) may be found in patients with heart disease and occasionally in
patients with chronic obstructive pulmonary dis-ease (COPD); dyspnea with an
expiratory wheeze occurs with COPD. Noisy breathing may result from a narrowing
of the air-way or localized obstruction of a major bronchus by a tumor or
foreign body. The presence of both inspiratory and expiratory wheezing usually
signifies asthma if the patient does not have heart failure.
The
circumstance that produces the dyspnea must be deter-mined. Therefore, it is
important to ask the patient the following questions:
·
How much exertion triggers shortness
of breath?
·
Is there an associated cough?
·
Is dyspnea related to other
symptoms?
·
Was the onset of shortness of breath
sudden or gradual?
·
At what time of day or night does
the dyspnea occur?
·
Is the shortness of breath worse
when the patient is flat in bed?
·
Does the shortness of breath occur
at rest? With exercise? Running? Climbing stairs?
· Is the shortness of breath worse while walking? If so, when walking how far? How fast?
Relief Measures.
The
management of dyspnea is aimed at iden-tifying and correcting its cause. Relief
of the symptom sometimes is achieved by placing the patient at rest with the
head elevated (high Fowler’s position) and, in severe cases, by administering
oxygen.
COUGH
Cough
results from irritation of the mucous membranes any-where in the respiratory
tract. The stimulus producing a cough may arise from an infectious process or
from an airborne irritant, such as smoke, smog, dust, or a gas. The cough is
the patient’s chief protection against the accumulation of secretions in the
bronchi and bronchioles.
Clinical Significance.
Cough may indicate serious pulmonarydisease. The nurse needs to evaluate the character of the cough— is it dry, hacking, brassy, wheezing, loose, or severe? A dry, irrita-tive cough is characteristic of an upper respiratory tract infection of viral origin or may be a side effect of angiotensin-converting enzyme (ACE) inhibitor therapy. Laryngotracheitis causes an ir-ritative, high-pitched cough. Tracheal lesions produce a brassy cough. A severe or changing cough may indicate bronchogenic carcinoma. Pleuritic chest pain accompanying coughing may in-dicate pleural or chest wall (musculoskeletal) involvement.
The time of coughing is also noted.
Coughing at night may herald the onset of left-sided heart failure or bronchial
asthma. A cough in the morning with sputum production may indicate bronchitis.
A cough that worsens when the patient is supine sug-gests postnasal drip
(sinusitis). Coughing after food intake may indicate aspiration of material
into the tracheobronchial tree. A cough of recent onset is usually from an
acute infection.
SPUTUM PRODUCTION
A patient who coughs long enough almost invariably produces sputum. Violent coughing causes bronchial spasm, obstruction, and further irritation of the bronchi and may result in syncope (fainting). A severe, repeated, or uncontrolled cough that is non-productive is exhausting and potentially harmful. Sputum production is the reaction of the lungs to any constantly recurring irritant. It also may be associated with a nasal discharge.
Clinical Significance.
A profuse amount of purulent sputum(thick and yellow, green, or rust-colored) or a change in color of the sputum probably indicates a bacterial infection. Thin, mu-coid sputum frequently results from viral bronchitis. A gradual increase of sputum over time may indicate the presence of chronic bronchitis or bronchiectasis. Pink-tinged mucoid sputum suggests a lung tumor. Profuse, frothy, pink material, often welling up into the throat, may indicate pulmonary edema. Foul-smelling sputum and bad breath point to the presence of a lung abscess, bronchiectasis, or an infection caused by fusospirochetal or other anaerobic organisms.
Relief Measures.
If
the sputum is too thick for the patient to ex-pectorate, it is necessary to
decrease its viscosity by increasing its water content through adequate
hydration (drinking water) and inhalation of aerosolized solutions, which may
be delivered by any type of nebulizer. Strategies to assist the patient to
cough pro-ductively are discussed later.
Smoking
is contraindicated with excessive sputum production because it interferes with
ciliary action, increases bronchial secre-tions, causes inflammation and
hyperplasia of the mucous mem-branes, and reduces production of surfactant.
Thus, smoking impairs bronchial drainage. When the person stops smoking, sputum
volume decreases and resistance to bronchial infections increases.
The
patient’s appetite may decrease because of the odor of the sputum or the taste
it leaves in the mouth. The nurse encourages adequate oral hygiene and wise
selection of food, measures that will stimulate appetite. In addition, the nurse
encourages the pa-tient and family to remove sputum cups, emesis basins, and
soiled tissues before mealtime. Encouraging the patient to drink citrus juices
at the beginning of the meal may increase the palatability of the rest of the
meal because these juices cleanse the palate of the sputum taste.
CHEST PAIN
Chest
pain or discomfort may be associated with pulmonary or car-diac disease. Chest
pain associated with pulmonary conditions may be sharp, stabbing, and
intermittent, or it may be dull, aching, and persistent. The pain usually is
felt on the side where the pathologic process is located, but it may be
referred elsewhere—for example, to the neck, back, or abdomen.
Clinical Significance.
Chest pain may occur with pneumonia,pulmonary embolism with lung
infarction, and pleurisy. It also may be a late symptom of bronchogenic
carcinoma. In carcinoma the pain may be dull and persistent because the cancer
has in-vaded the chest wall, mediastinum, or spine.
Lung
disease does not always produce thoracic pain because the lungs and the
visceral pleura lack sensory nerves and are in-sensitive to pain stimuli.
However, the parietal pleura has a rich supply of sensory nerves that are
stimulated by inflammation and stretching of the membrane. Pleuritic pain from irritation
of the parietal pleura is sharp and seems to “catch” on inspiration; pa-tients
often describe it as “like the stabbing of a knife.” Patients are more
comfortable when they lie on the affected side as this splints the chest wall,
limits expansion and contraction of the lung, and reduces the friction between
the injured or diseased pleurae on that side. Pain associated with cough may be
reduced manually by splinting the rib cage.
The
nurse assesses the quality, intensity, and radiation of pain and identifies and
explores precipitating factors, along with their relationship to the patient’s
position. Also, it is important to as-sess the relationship of pain to the
inspiratory and expiratory phases of respiration.
Relief Measures.
Analgesic
medications may be effective in re-lieving chest pain, but care must be taken
not to depress the respiratory center or a productive cough, if present.
Nonsteroidal anti-inflammatory drugs (NSAIDs) achieve this goal and thus are
used for pleuritic pain. A regional anesthetic block may be per-formed to
relieve extreme pain.
WHEEZING
Wheezing
is often the major finding in a patient with bron-choconstriction or airway
narrowing. It is heard with or without a stethoscope, depending on its
location. Wheezing is a high-pitched, musical sound heard mainly on expiration.
Relief Measures. Oral
or inhalant bronchodilator medicationsreverse wheezing in most instances.
CLUBBING OF THE FINGERS
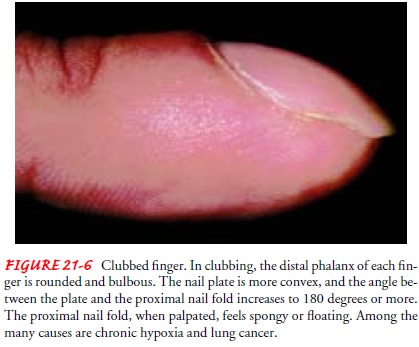
Clubbing
of the fingers is a sign of lung disease found in patients with chronic hypoxic
conditions, chronic lung infections, and ma-lignancies of the lung. This
finding may be manifested initially as sponginess of the nailbed and loss of
the nailbed angle (Fig. 21-6).
HEMOPTYSIS
Hemoptysis (expectoration of blood from the respiratory tract) is a symptom of both pulmonary and cardiac disorders. The onset of hemoptysis is usually sudden, and it may be intermittent or continuous. Signs, which vary from blood-stained sputum to a large, sudden hemorrhage, always merit investigation. The most common causes are:
·
Pulmonary infection
·
Carcinoma of the lung
·
Abnormalities of the heart or blood
vessels
·
Pulmonary artery or vein
abnormalities
·
Pulmonary emboli and infarction
Diagnostic
evaluation to determine the cause includes several studies: chest x-ray, chest
angiography, and bronchoscopy. A care-ful history and physical examination are
necessary to diagnose the underlying disease, irrespective of whether the
bleeding involved a very small amount of blood in the sputum or a massive
hemor-rhage. The amount of blood produced is not always proportional to the
seriousness of the cause.
First,
it is important to determine the source of the bleeding— the gums, nasopharynx,
lungs, or stomach. The nurse may be the only witness to the episode. When
documenting the bleeding episode, the nurse considers the following points:
·
Bloody sputum from the nose or the
nasopharynx is usually preceded by considerable sniffing, with blood possibly
ap-pearing in the nose.
·
Blood from the lung is usually
bright red, frothy, and mixed with sputum. Initial symptoms include a tickling
sensation in the throat, a salty taste, a burning or bubbling sensation in the
chest, and perhaps chest pain, in which case the pa-tient tends to splint the bleeding
side. The term “hemop-tysis” is reserved for the coughing up of blood arising
from a pulmonary hemorrhage. This blood has an alkaline pH (greater than 7.0).
·
If the hemorrhage is in the stomach,
the blood is vomited (hematemesis) rather than coughed up. Blood that has been
in contact with gastric juice is sometimes so dark that it is referred to as
“coffee grounds.” This blood has an acid pH (less than 7.0).
CYANOSIS
Cyanosis,
a bluish coloring of the skin, is a very late indicator of hypoxia. The
presence or absence of cyanosis is determined by the amount of unoxygenated
hemoglobin in the blood. Cyanosis ap-pears when there is 5 g/dL of unoxygenated
hemoglobin. A pa-tient with a hemoglobin level of 15 g/dL will not demonstrate
cyanosis until 5 g/dL of that hemoglobin becomes unoxygenated, reducing the
effective circulating hemoglobin to two thirds of the normal level. An anemic
patient rarely manifests cyanosis, and a polycythemic patient may appear
cyanotic even if adequately oxygenated. Therefore, cyanosis is not a reliable sign of hypoxia.
Assessment
of cyanosis is affected by room lighting, the pa-tient’s skin color, and the
distance of the blood vessels from the surface of the skin. In the presence of
a pulmonary condition, central cyanosis is assessed by observing the color of
the tongue and lips. This indicates a decrease in oxygen tension in the blood.
Peripheral cyanosis results from decreased blood flow to a certain area of the
body, as in vasoconstriction of the nailbeds or earlobes from exposure to cold,
and does not necessarily indicate a central systemic problem.
Related Topics