Chapter: Medicine and surgery: Genitourinary system
Glomerular disease
Glomerular disease
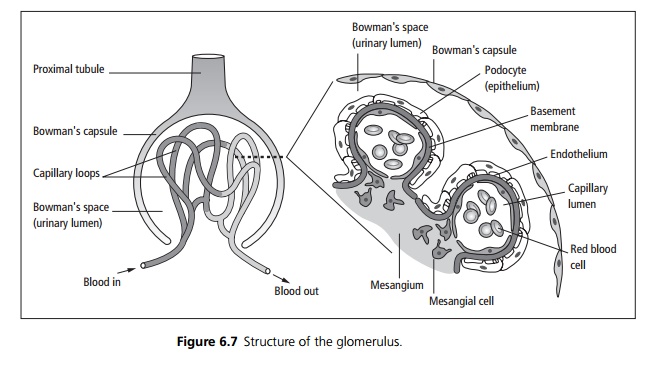
The glomerulus is an intricate structure, the function of which depends
on all its constituent parts being intact (see Fig. 6.7).
1.
Blood reaches the glomerular
capillary system via the afferent arteriole. On the vascular side of the
barrier between the blood and the filtrate is endothe-lium, fused to the
glomerular basement membrane (GBM). On the filtrate side is an epithelium
composed of podocytes, attached to the GBM by foot processes. The connective
tissue, which supports the capillary network, is called ŌĆśmesangiumŌĆÖ.
2.
The pressure in the glomerular
capillaries is higher than that in the urinary lumen, so that constituents of
the blood are filtered into the urinary lumen. This ŌĆśultrafiltrateŌĆÖ is almost
an exact mirror of plasma except for proteins because the GBM is relatively
impermeable to high molecular weight proteins such as albumin. It is also less
permeable to negatively charged molecules.
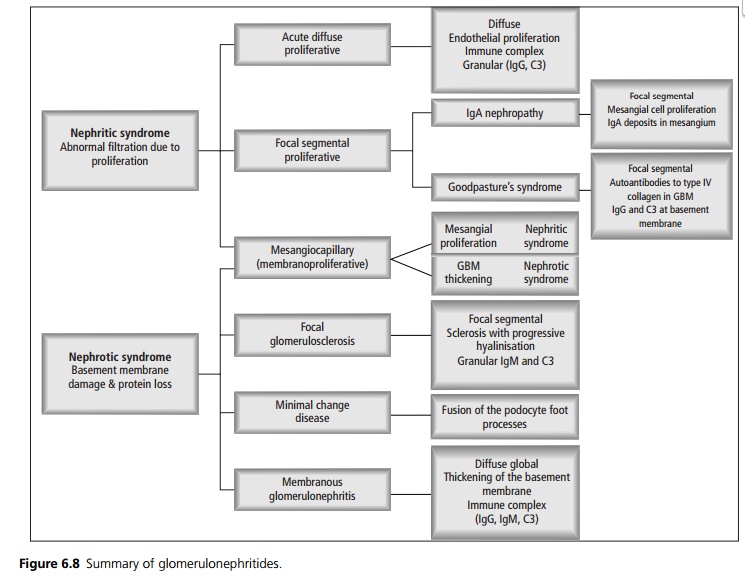
There are three main types of glomerular disease:
┬Ę
Glomerulonephritis describes a
variety of conditions characterised by inflammation of glomeruli in both
kidneys, which have an immunological basis.
┬Ę
Vasculitis which can mimic
glomerulonephritis, by damage to the glomerular vessels.
┬Ę
Glomerular damage may also occur
due to infiltration by abnormal material, such as by amyloid.
The type of damage caused to the structure of the glomerulus determines
the pathological appearance, has a broad relationship to the effect on renal
function and hence the clinical presentation. The disease process may be
diffuse affecting all the glomeruli, or focal affecting only some of the
glomeruli. Affected glomeruli may be completely damaged (global), or only a part
may be damaged (segmental). Most glomerular diseases are either diffuse global
or focal segmental.
Within the glomerulus itself, there are different appearances:
┬Ę
Proliferation of endothelial
cells and mesangial cells is common in diseases that cause nephritic syndrome
(see Fig. 6.8). Endothelial cell proliferation leads to occlusion of the
capillary lumen, reduced blood flow, oliguria and acute renal failure.
Mesangial cell proliferation, which is usually associated with increased
production of mesangial matrix, can lead to scarring (sclerosis) of all or part
of the glomerulus. Increased matrix can lead to reduced blood flow and/or
proteinuria.
┬Ę
GBM thickening, which can be due
to a number of mechanisms, tends to cause nephrotic syndrome, and can be due to
a number of mechanisms (often coexistent) including deposition of immune
complexes, oversynthesis of basement membrane material and ingrowth of
mesangium.
┬Ę
More severe patterns may occur
when the glomerular capillary walls are acutely and severely damaged.
┬Ę
Fibrinoid necrosis, where fibrin
is deposited in the necrotic vessel walls. Crescents are formed when necrotic
vessel walls leak blood and fibrin, so that macrophages and proliferating
epithelial cells invade the BowmanŌĆÖs space, crushing the glomerulus. If there
are crescents in most of the glomeruli, the term rapidly progressive
glomerulonephritis is used, as severe rapid onset acute renal failure usually
results.
┬Ę
Almost all forms of
glomerulonephritis have a cellular or humoral immunological basis:
┬Ę
Humoral response: Immune deposits
(antibodies or antibodyŌĆōantigen complexes) in the glomerulus fix and activate
complement and a variety of other inflammatory mediators such as antioxidants,
proteases and cytokines. The sites, number and type of deposits determine the
type and extent of damage caused. Mesangial deposits cause mesangial cell
proliferation and increased mesangial matrix. Subendothelial deposits are close
to the glomerular capillary lumen, so excite marked inflammation which can lead
to rapidly progressive glomerular nephritis, whereas subepithelial deposits
excite less of an inflammatory response, because the glomerular basement
membrane prevents the influx of cells from the capillaries. Circulating immune
complexes filtered by the kidney tend to cause less injury than complexes
formed de novo in the glomerulus.
┬Ę
Cellular response: Some
glomerular diseases (such as minimal change nephropathy and focal segmental glomerulosclerosis) show little or no antibody
deposition. It appears that lymphocytes, in particular T cells play a role in
causing the functional changes.
┬Ę
Macrophages: These may be
involved in both humoral and cellular pathways.
Immunofluorescence and electron
microscopy: The diagnosis of glomerular
disease may not be possible with light microscopy only. Immunofluorescence is
used to look for immune complex and C3 and C4 deposits and electron microscopy is also used.
Related Topics