Chapter: Medical Physiology: The Eye: I. Optics of Vision
Fluid System of the Eye- Intraocular Fluid
Fluid System of the Eye- Intraocular Fluid
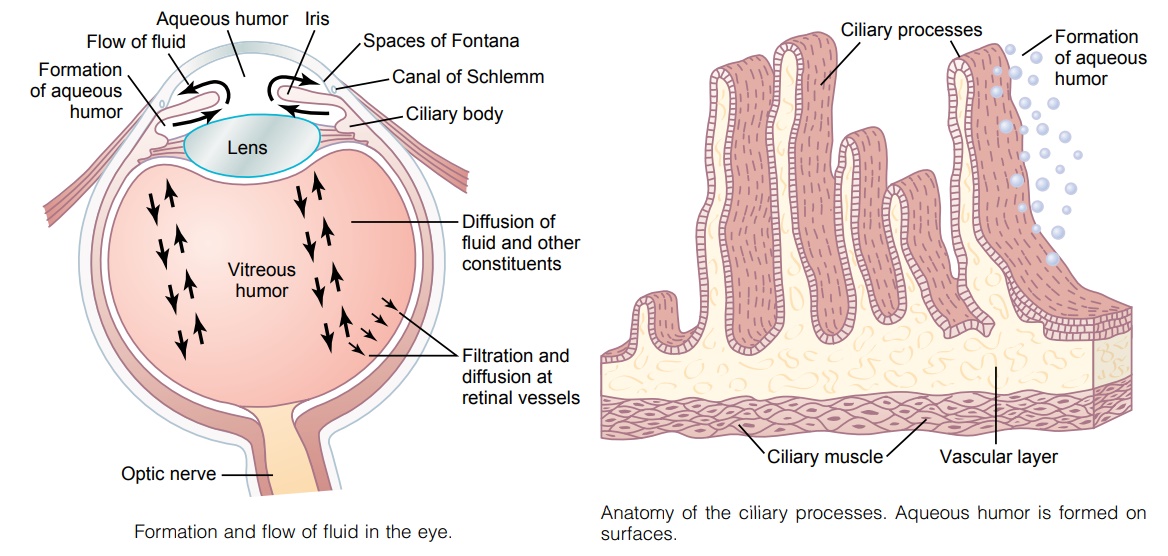
The eye is filled with intraocular fluid, which maintains sufficient pressure in the eyeball to keep it distended. Figure 49–19 demonstrates that this fluid can be divided into two portions—aqueous humor, which lies in front of the lens, and vitreous humor, which is between the posterior surface of the lens and the retina. The aqueous humor is a freely flowing fluid, whereas the vitreous humor, sometimes called the vitreous body, is a gelati-nous mass held together by a fine fibrillar network com-posed primarily of greatly elongated proteoglycan molecules. Both water and dissolved substances can diffuse slowly in the vitreous humor, but there is little flow offluid.
Aqueous humor is continually being formed and reabsorbed. The balance between formation and reab-sorption of aqueous humor regulates the total volume and pressure of the intraocular fluid.
Formation of Aqueous Humor by the Ciliary Body
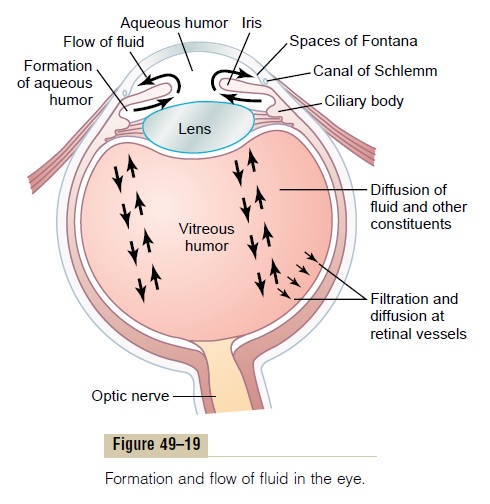
Aqueous humor is formed in the eye at an average rateof 2 to 3 microliters each minute. Essentially all of it issecreted by the ciliary processes, which are linear folds projecting from the ciliary body into the space behind the iris where the lens ligaments and ciliary muscle attach to the eyeball. A cross section of these ciliary processes is shown in Figure 49–20, and their relation to the fluid chambers of the eye can be seen in Figure 49–19. Because of their folded architecture, the total surface area of the ciliary processes is about 6 square centimeters in each eye—a large area, considering the small size of the ciliary body. The surfaces of these processes are covered by highly secretory epithelial cells, and immediately beneath them is a highly vascu-lar area.
Aqueous humor is formed almost entirely as an active secretion by the epithelium of the ciliary processes. Secretion begins with active transport of sodium ions into the spaces between the epithelial cells. The sodium ions pull chloride and bicarbonate ions along with them to maintain electrical neutrality. Then all these ions together cause osmosis of water from the blood capil-laries lying below into the same epithelial intercellular spaces, and the resulting solution washes from the spaces of the ciliary processes into the anterior chamber of the eye. In addition, several nutrients are transported across the epithelium by active transport or facilitated diffusion; they include amino acids, ascorbic acid, and glucose.
Outflow of Aqueous Humor from the Eye
After aqueous humor is formed by the ciliary processes, it first flows, as shown in Figure 49–19, through the pupilinto the anterior chamber of the eye. From here, thefluidflows anterior to the lens and into the angle between the
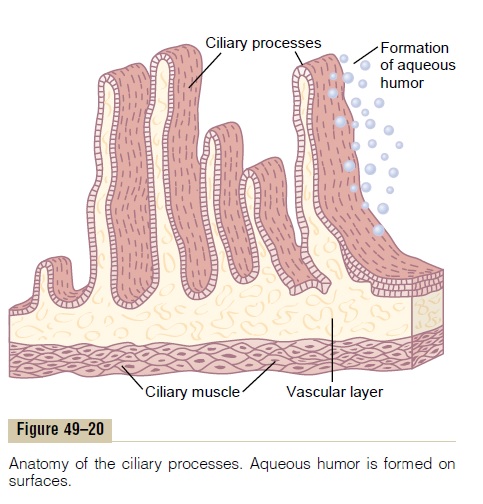
Figure 49–21 demon-strates the anatomical structures at this iridocorneal angle, showing that the spaces between the trabeculae extend all the way from the anterior chamber to the canal of Schlemm. The canal of Schlemm is a thin-walled vein that extends circumferentially all the way around the eye. Its endothelial membrane is so porous that even large protein molecules, as well as small par-ticulate matter up to the size of red blood cells, can pass from the anterior chamber into the canal of Schlemm. Even though the canal of Schlemm is actually a venous blood vessel, so much aqueous humor normally flows into it that it is filled only with aqueous humor rather than with blood. The small veins that lead from the canal of Schlemm to the larger veins of the eye usually contain only aqueous humor, and they are called aqueous veins.
Intraocular Pressure
The average normal intraocular pressure is about 15 mm Hg, with a range from 12 to 20 mm Hg.
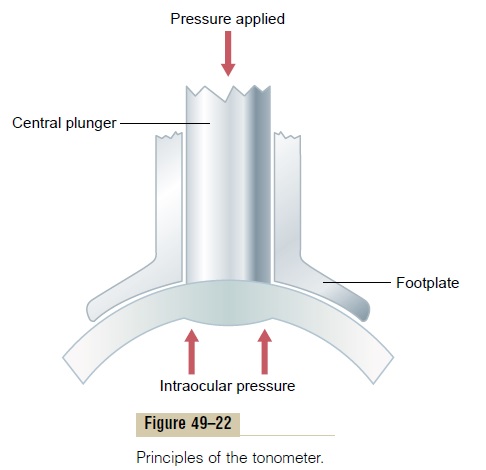
Tonometry. Because it is impractical to pass a needle intoa patient’s eye to measure intraocular pressure, this pressure is measured clinically by using a “tonometer,” the principle of which is shown in Figure 49–22. The cornea of the eye is anesthetized with a local anesthetic, and the footplate of the tonometer is placed on the cornea. A small force is then applied to a central plunger, causing the part of the cornea beneath the plunger to be displaced inward. The amount of dis-placement is recorded on the scale of the tonometer, and this is calibrated in terms of intraocular pressure.
Regulation of Intraocular Pressure. Intraocular pressureremains constant in the normal eye, usually within ±2 mm Hg of its normal level, which averages about 15 mm Hg. The level of this pressure is determined mainly by the resistance to outflow of aqueous humor from the anterior chamber into the canal of Schlemm.
This outflow resistance results from the meshwork of trabeculae through which the fluid must percolate on its way from the lateral angles of the anterior chamber to the wall of the canal of Schlemm. These trabeculae have minute openings of only 2 to 3 micrometers. The rate of fluid flow into the canal increases markedly as the pres-sure rises. At about 15 mm Hg in the normal eye, the amount of fluid leaving the eye by way of the canal of Schlemm usually averages 2.5 ml/min and equals the inflow of fluid from the ciliary body. The pressure nor-mally remains at about this level of 15 mm Hg.
Mechanism for Cleansing the Trabecular Spaces and Intraocular Fluid. When large amounts of debris are present in theaqueous humor, as occurs after hemorrhage into the eye or during intraocular infection, the debris is likely to accumulate in the trabecular spaces leading from the anterior chamber to the canal of Schlemm; this debris can prevent adequate reabsorption of fluid from the anterior chamber, sometimes causing “glaucoma,” as explained subsequently. However, on the surfaces of the trabecular plates are large numbers of phagocytic cells. Immediately outside the canal of Schlemm is a layer of interstitial gel that contains large numbers of reticu-loendothelial cells that have an extremely high capacity for engulfing debris and digesting it into small molecu-lar substances that can then be absorbed. Thus, this phagocytic system keeps the trabecular spaces cleaned. The surface of the iris and other surfaces of the eye behind the iris are covered with an epithelium that is capable of phagocytizing proteins and small particles from the aqueous humor, thereby helping to maintain a clear fluid.
“Glaucoma,” a Principal Cause of Blindness. Glaucoma is oneof the most common causes of blindness. It is a disease of the eye in which the intraocular pressure becomes pathologically high, sometimes rising acutely to 60 to 70 mm Hg. Pressures above 25 to 30 mm Hg can cause loss of vision when maintained for long periods. Extremely high pressures can cause blindness within days or even hours. As the pressure rises, the axons of the optic nerve are compressed where they leave the eyeball at the optic disc. This compression is believed to block axonal flow of cytoplasm from the retinal neu-ronal cell bodies into the optic nerve fibers leading to the brain. The result is lack of appropriate nutrition of the fibers, which eventually causes death of the involved fibers. It is possible that compression of the retinal artery, which enters the eyeball at the optic disc, also adds to the neuronal damage by reducing nutrition to the retina.
In most cases of glaucoma, the abnormally high pres-sure results from increased resistance to fluid outflow through the trabecular spaces into the canal of Schlemm at the iridocorneal junction. For instance, in acute eye inflammation, white blood cells and tissue debris can block these trabecular spaces and cause an acute increase in intraocular pressure. In chronic conditions, especially in older individuals, fibrous occlusion of the trabecular spaces appears to be the likely culprit.
Glaucoma can sometimes be treated by placing drops in the eye that contain a drug that diffuses into the eyeball and reduces the secretion or increases the absorption of aqueous humor. When drug therapy fails, operative techniques to open the spaces of the trabec-ulae or to make channels to allow fluid to flow directly from the fluid space of the eyeball into the subconjunc-tival space outside the eyeball can often effectively reduce the pressure.
Related Topics