Chapter: Medicine Study Notes : Haematology and Immunology
Fever in a Neutropenic Patient
Fever in a Neutropenic Patient
· Eg in patients undergoing chemotherapy
· Indicators of serious infection:
o Signs and symptoms of infection will be reduced – can‟t mount an inflammatory response
o Temperature:
§ > 38.5 C
§ > 38 for 4 hours
§ Patient fells unwell but no temperature
o Neutropenia:
§ Neutrophils < 0.5 * 10E9/L (less than 0.2 Þ serious concern)
§ Neutrophils falling
§ Prolonged neutropenia (> 7 days)
· Types of infection (drives focused history)
o Respiratory: SOB, cough
o Skin infection
o Mouth and teeth
o Perianal (pain on moving bowels and wiping)
o Pain around central line
o Less often: bowel & UTI
· Focused exam:
o Signs of septic shock: Pulse, BP and peripheral circulation
o Chest: percussion and auscultation
o Mouth: a good look around – abscesses will be sensitive to pain
o Skin infections, especially lines
o Quick abdominal
o Exam perianal area – test for sensitivity to touch. Don‟t do PR (risk of minor trauma ® bacteraemia)
· Investigations:
o FBC
o Blood culture (debate about whether to take it from the central line or not)
o CXR
o Swabs from anything that looks infected, including central line
o Maybe CRP: in bacteraemia
· Normally don‟t find anything. Over half infections are low grade line infections
· If in doubt, treat empirically now. If infected will deteriorate quickly:
o Gentamycin + Ticarcillin (synthetic penicillin)
o Monotherapy (eg imipenem)
o +/- Vancomycin (for staph line sepsis)
· Causes of infection:
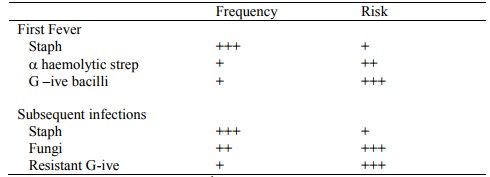
· Subsequent fevers: longer in hospital (hospital acquired infection), longer on antibiotics, etc
· If fever persists:
o Repeat the above exam and investigations – but unlikely to add anything new
o Choices:
§ Change antibiotics
§ Consider antifungal: Amphotericin. Watch for nephrotoxicity and the patient feels awful
· Obscure fevers:
o Central venous line infection
o Occult sinusitis (check with CT)
o Hepatosplenic candidiasis (check with CT ® abscess ® biopsy)
o Pulmonary/disseminated aspergillus (doesn‟t respond to amphotericin)
o Viral
o Drugs
· Prevention:
o Avoid hospitalisation
o Strict hand washing
o Avoid invasive procedures (beware interventionist surgeons!)
o Care of IV devices
o Consider prophylactic antimicrobials
· Prophylaxis
o Bacteria: selective gut decontamination (origin of many infections is bowel flora): Ciprofloxacin (fluorinated quinolone). Arguments for and against
o Anti-fungal: Fluconazole, Itraconazole (OK for prophylaxis, not so good as amphotericin for established infection)
o Anti-viral: acyclovir (for HSV), ganciclovir (for CMV)
o Anti-pneumocystis: co-trimoxazole (but beware marrow suppression) or aerolised pentamidine
· Other possible treatments:
o Granulocyte-CSF: try to marrow production of neutrophils
o Maybe g-globulin infusions
o Transfuse granulocytes: emerging area
Related Topics