Chapter: Basic Radiology : Gastrointestinal Tract
Exercise: Upper Gastrointestinal Bleeding
EXERCISE 10-2.
UPPER GASTROINTESTINAL BLEEDING
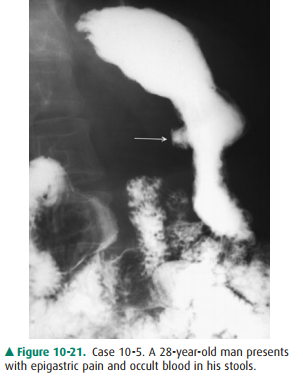
10-5. What is the most likely cause of the lesser curvature gastric lesion (arrow) shown in Case 10-5 (Figure 10-21)?
A.
Malignant gastric ulcer
B.
Gastric diverticulum
C.
Lymphoma of the stomach
D.
Polypoid carcinoma of the stomach
E.
Benign gastric ulcer
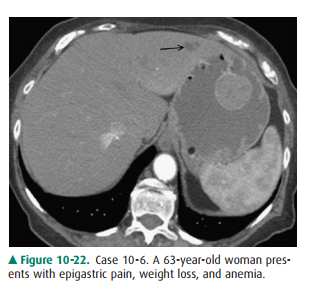
10-6. What is the least likely cause of the polypoid gastric mass shown in Case 10-6 (Figure
10-22)?
A.
Large gastric adenoma
B.
GIST (gastrointestinal stromal tumor)
C.
Gastric lymphoma
D.
Polypoid gastric carcinoma
E.
Gastric leiomyosarcoma.
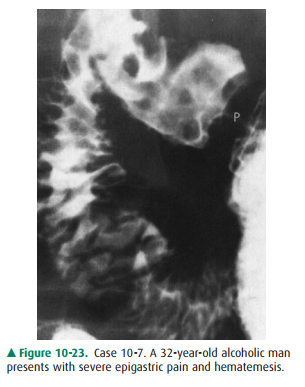
10-7. What is the likely diagnosis for the nodular
appearance of the duodenal bulb in Case 10-7
(Figure 10-23; p, pylorus)?
A.
Duodenal ulcer
B.
Erosive duodenitis
C.
Brunner gland hyperplasia
D.
Duodenal carcinoma
E.
Swallowed olive pits
10-8. What is the most likely cause of the barium collection in the duodenal bulb in Case 10-8 (Figure 10-24; pa-tient is
prone; d, duodenal diverticulum)?

A.
Benign duodenal ulcer (posterior wall)
B.
Malignant duodenal ulcer
C.
Benign duodenal polyp
D.
Benign duodenal ulcer (anterior wall)
E.
Ulcerated duodenal metastasis
Radiologic Findings
10-5. A smooth barium collection projects from the lesser curvature of the stomach and is associated with a lucent
“collar” at the neck of the collection, a combination of findings most
consistent with benign gastric ulcer (E is the correct answer to Question
10-5).
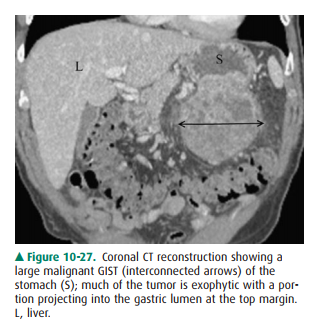
10-6. A polypoid lesion in the stomach is most likely a gas-tric
neoplasm; the size of the lesion and the presence of a left lobe liver
metastasis (arrow) would suggest a malignancy; a GI stromal tumor was diagnosed
on pathologic examination (A is the correct answer to Question 10-6).
10-7. Multiple nodules are present in the duodenal bulb, some with central collections of barium, most indica-tive of
duodenal erosions (B is the correct answer to Question 10-7).
10-8. The central collection of barium in the duodenal bulb is located on the anterior wall with the patient prone, thus
localizing the lesion; duodenal ulcer with sur-rounding edema was seen at
endoscopy (D is the cor-rect answer to Question 10-8).
Discussion
Many causes of upper
gastrointestinal bleeding can be de-tected on a radiographic examination of
this portion of the gastrointestinal tract. As illustrated in the cases of this
exer-cise, the most important causes are gastric or duodenal ero-sions and
ulcers, and neoplasms of the stomach.
The radiographic features that
suggest a benign gastric ulcer include (1) projection from the lumen of the
stomach;smooth lucent line (Hampton line) or collar (as in this case) at the
neck of the ulcer; (3) normal rugal folds that ra-diate to the edge of the
ulcer collection; and (4) complete and permanent healing of the ulcer on repeat
radiographic or en-doscopic examination of the stomach. If at least two or more
of these findings are present, a confident radiographic diag-nosis of benign
gastric ulcer is possible. A malignant gastric ulcer, which represents a small
minority of all ulcers seen in the stomach, is suggested when the collection of
barium within the ulcer is irregular and projects within the gastric lumen (ie,
ulcerated neoplastic mass), a smooth line or collar at the ulcer margin is not
present, or the rugal folds are nodu-lar and terminate abruptly (Figure 10-25).
Lack of healing of a gastric ulcer is not a specific sign of malignancy.

Adenocarcinoma remains the most
common primary ma-lignancy of the stomach, but its incidence has decreased
dra-matically in the United States. Gastric adenocarcinoma comprises about 95%
of all primary malignancies of the stomach; lymphoma and GI stromal tumors
account for most of the remainder. These gastric neoplasms show a wide variety
of morphologic forms that include ulcerative, polypoid, infil-trative, or mixed
varieties, depending on the type of tumor
GIST is the most
common mesenchymal tumor of the stomach and arises from the pacemaker cells of
Cajal in the muscularis propria; special stains are used to make a specific
diagnosis. GI stromal tumors may be small and polypoid, resembling benign
gastric polyps; larger le-sions are often ulcerated and reveal malignant
features, such as local invasion and metastases. GIST may be endoluminal or
exophytic in location (Figure 10-27), although both com-ponents may be present
(“dumbbell tumors”).
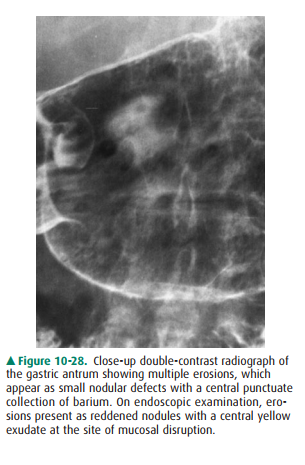
Erosions in the stomach and
duodenum are a common cause of upper gastrointestinal bleeding. Because these
ero-sions may be few in number and small in size, endoscopic ex-amination of
the stomach and duodenum is more sensitive in their detection than radiologic
evaluation. The radiographic features of duodenitis depend on the severity of
the disease and include thickening and nodularity of the duodenal folds or the
presence of erosions, which appear as punctuate collections of barium centered
on a nodule. Brunner gland hyperplasia may have an appearance similar to
duodenitis, but erosions are not seen, and patients may not be symptomatic.
Carcinoma of the duodenal bulb is extremely rare and does not typically enter
the differential diagnosis of inflammatory lesions in this anatomic region.
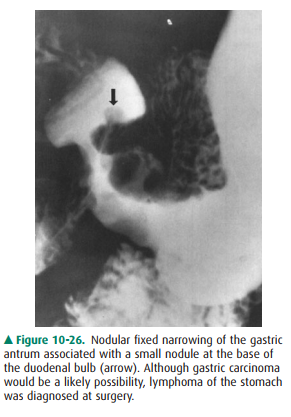
Gastric erosions also appear as nodular de-fects, usually in the antrum of the
stomach (Figure 10-28).
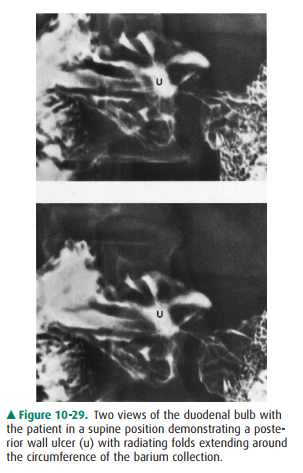
Approximately 95% of duodenal ulcers
occur within the duodenal bulb and have about an equal distribution on the
an-terior and posterior walls of the duodenum. The remaining 5% of duodenal
ulcers are located near the apex of the bulb. On radiographic examination, a
duodenal ulcer is seen as a round or oval collection of barium that should
maintain a fixed size and shape on multiple images of the collection;
inconsistent collections of barium, often seen in the duodenal fornices or at
the apex or in the presence of bulbar deformity, may be mistaken for an active
ulcer. Anterior wall duodenal ulcers are best visualized with the patient in
the prone position (as in this case), whereas posterior wall ulcers are seen
well with the patient supine (Figure 10-29). As with duodenal carcino-mas, polyps
in the duodenal bulb are rare and would appear as lucent filling defects and
not as a collection of barium.
Related Topics