Chapter: Basic Radiology : Radiology of the Chest
Exercise: Cavitary Disease
EXERCISE 4-9.
CAVITARY DISEASE
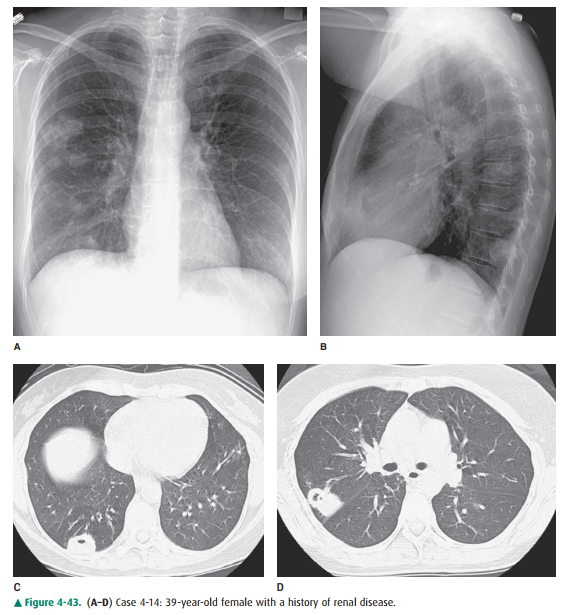
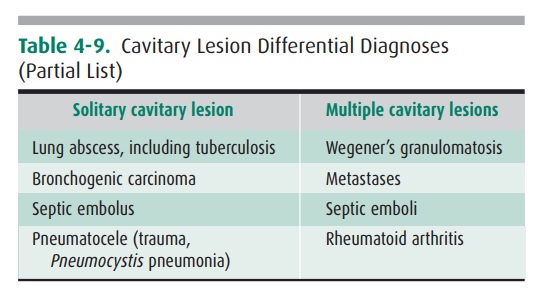
4-14. The chest
radiographic findings (Figure 4-43 A, B) in Case 4-14 could be best explained
as
A.
multiple lung abscesses due to Staphylococcus aureus.
B.
pneumatoceles due to Pneumocystis
jiroveci pneu-monia.
C.
Wegener’s granulomatosis.
D.
multiple cavities due to Mycobacterium
avium-intracellulare.
E.
metastases from Kaposi’s sarcoma.
Radiologic Findings
4-14. PA and lateral
chest radiographs (Figures 4-43 A,B) and CT images (Figure 4-43 C,D) show at
least two thick-walled cavitary lesions in the right lung (C is the correct
answer to Question 4-14). There is no hilar or mediastinal lymph node
enlargement. The heart and skeleton are normal.
Discussion
Inflammatory lesions are the most
common cause of lung cavities (Table 4-9). The number of cavities may range
from one to many. A wide variety of infecting organisms may re-sult in
cavitation, and the radiograph is nonspecific as to eti-ology. There is
considerable overlap in appearances from the various organisms, so that culture
or histologic evaluation is the only satisfactory means of identifying the
etiology. If the lesion is single, a cavitating pneumonia should be the first
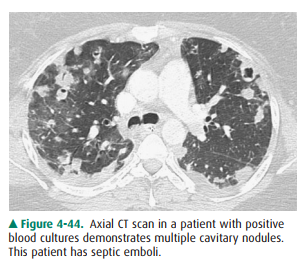
consideration, especially if the patient is febrile. If multiple cavities are
present (Figure 4-44), the infection is likely due to hematogenous
dissemination, and a source for this dissemi-nation should be sought. The
source could be right-sided en-docarditis or infected venous thrombi. Staphylococcus aureus pneumonias are
frequently seen in intravenous drug users and usually appear as multiple
cavities. These usually have thin walls (2 to 4 mm) that are slightly
indistinct on their outer borders.
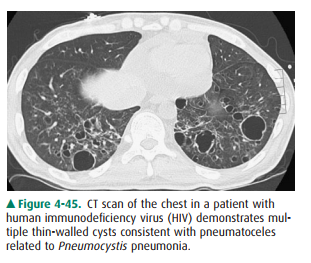
As the acquired immunodeficiency
syndrome (AIDS) epi-demic has progressed, it has been recognized that patients
with Pneumocystis jiroveci may
develop cavitary lesions in the lungs (Figure 4-45). These cavities may be
reversible and re-sult from pneumatoceles, or they may be due to a slowly
pro-gressive granulomatous reaction. The cavities are usually in the upper
lobes and are thin walled. Pneumothorax can result when a peripheral cavity
ruptures through the visceral pleura, into the pleural space.
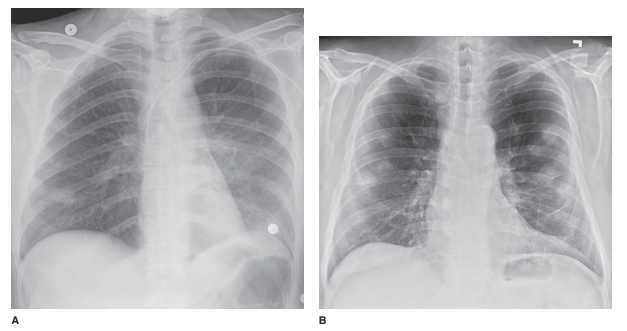
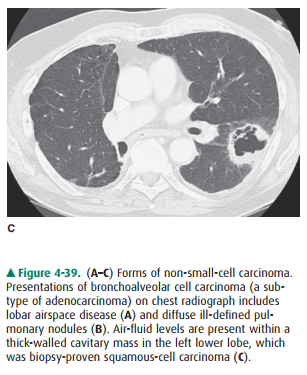
Neoplasia, either primary or
secondarily involving the lung, may also cavitate (see Figure 4-39 C). Cavities
may re- sult from pulmonary vasculitis, of which Wegener’s granulo-matosis is
the prototype. Demonstrating the importance of clinical history, the supplied
history of renal disease points toward Wegener’s granulomatosis.
Related Topics